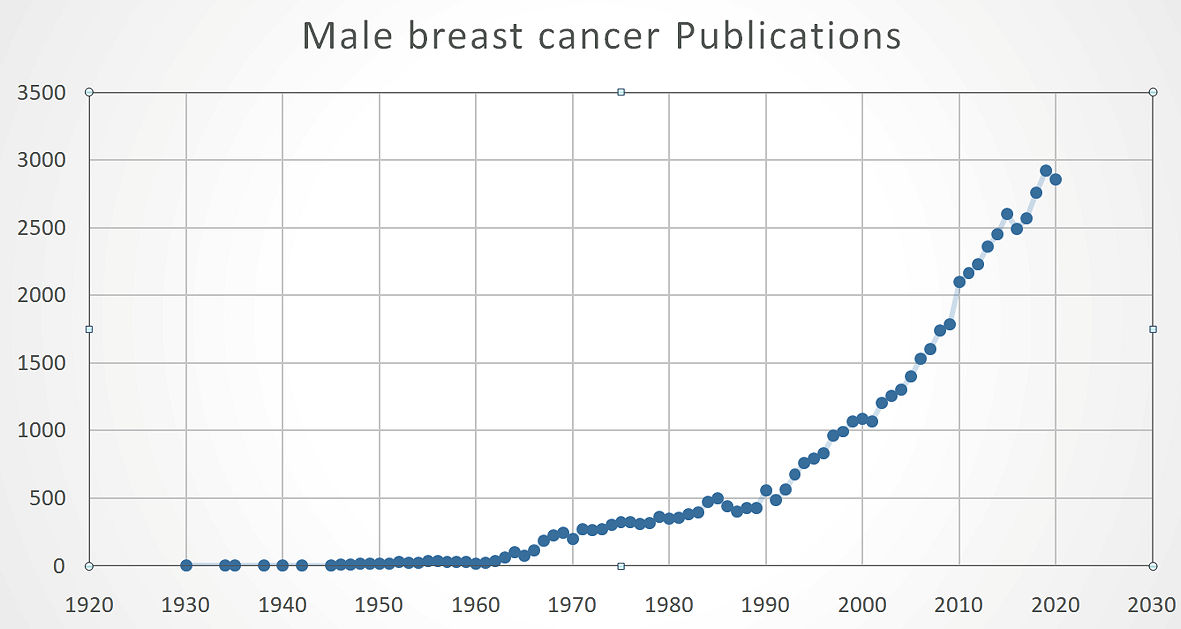
Figure 1. Publication trend for MaBC. MaBC: male breast cancer.
| World Journal of Oncology, ISSN 1920-4531 print, 1920-454X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Oncol and Elmer Press Inc |
| Journal website https://www.wjon.org |
Review
Volume 12, Number 6, December 2021, pages 206-213
Management of Male Breast Cancer: The Journey so Far and Future Directions
Figure
Table
| Surgery | Lumpectomy: feasible for very early disease and disease distant from the nipple-areolar complex | Surgery should be individualized but current mainstay of therapy is still mastectomy |
| Mastectomy: Most common surgery for MaBC | ||
| Surgery for axilla | Clinically negative lymph nodes should be assessed with sentinel lymph node biopsy | Lymph node staging is an integral step for therapy planning and completed based on clinical exam |
| Clinically positive lymph nodes can be biopsied radiographically | ||
| Radiation therapy | Adjuvant radiation therapy is recommended for stage I - III MaBC | Radiation oncology evaluation should be considered for all MaBC patients |
| Hormonal therapy | Tamoxifen: hormone-positive MaBC are recommended tamoxifen for 5 years with option to increase duration to 10 years | Majority of MaBC patients are candidates for hormone therapy with compliance being the biggest stumbling block |
| Aromatase inhibitors: prescribed in the recurrent of metastatic | ||
| Chemotherapy/targeted therapy | Cytotoxic chemotherapy has established role in MaBC | Chemotherapy is used in the adjuvant, neoadjuvant and palliative setting for MaBC |
| Trastuzumab for HER-2-positive patients can be exploited for additional survival benefit |