Figures
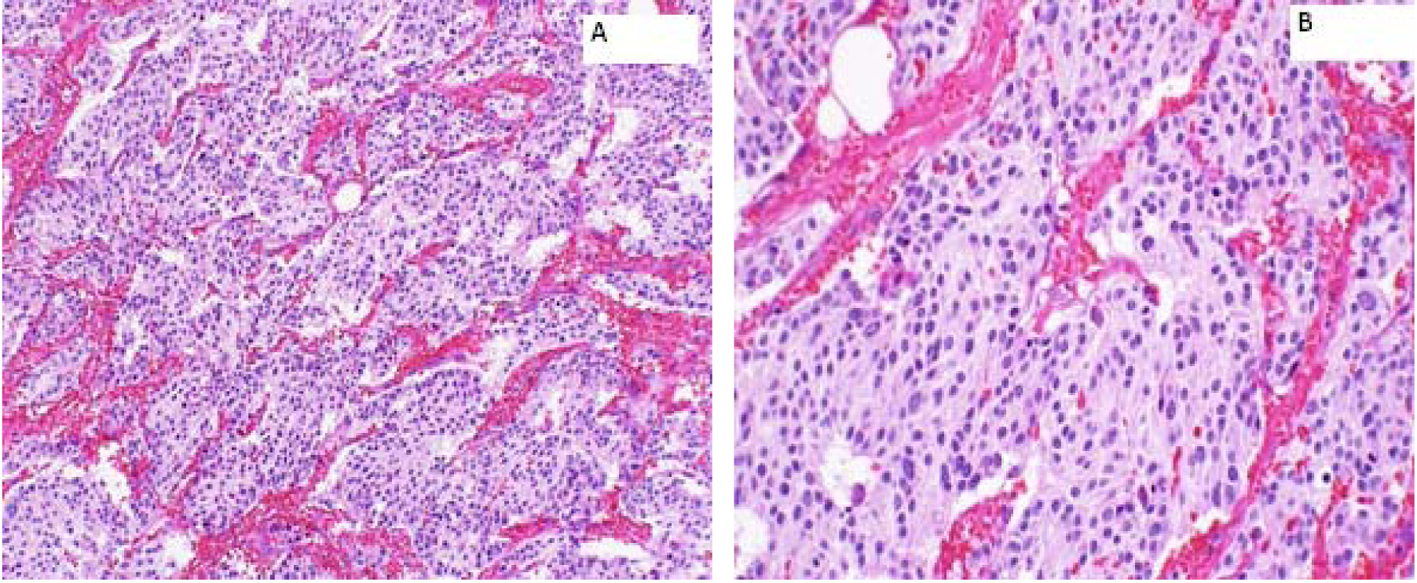
Figure 1. Right adrenal bed resection compatible with recurrent malignant pheochromocytomas. (A) × 100: microscopically, the tumor cells are arranged in well defined nests (“Zellballen”) bound by delicate fibrovascular stroma; (B) × 200: higher power shows amphophilic cytoplasm with a somewhat fibrillary cytoplasm.
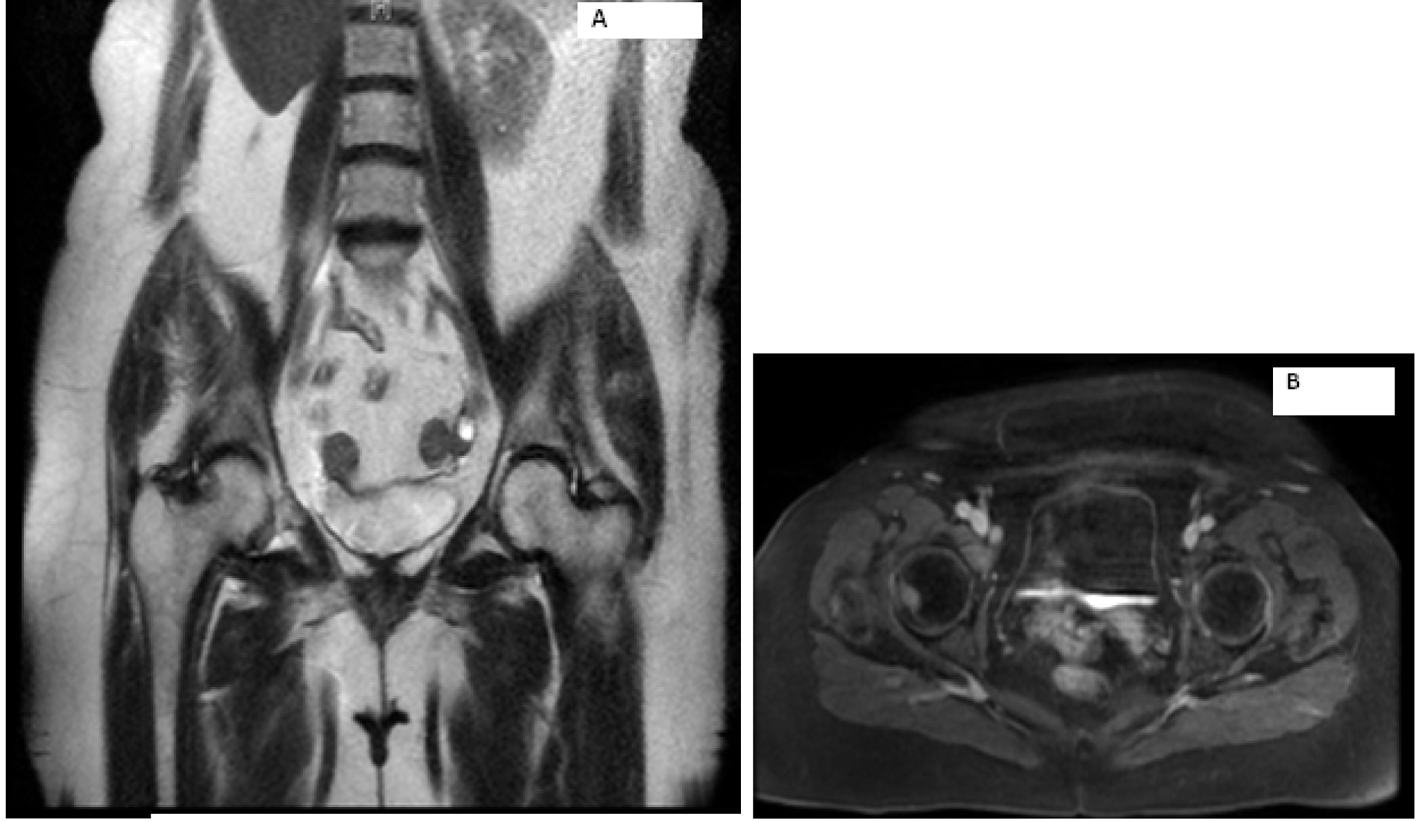
Figure 2. Magnetic resonance imaging of the abdomen showing metastasis to right hip.
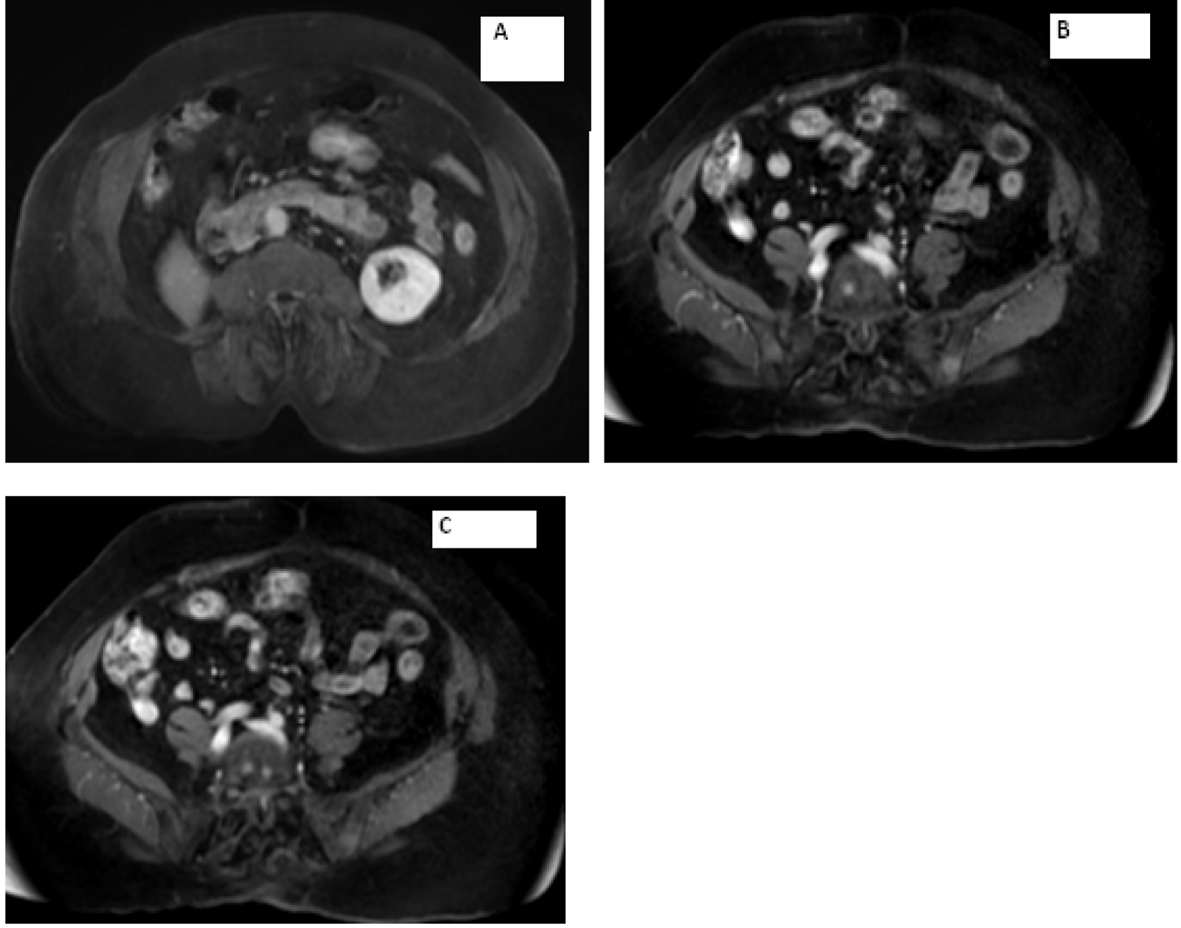
Figure 3. Magnetic resonance imaging of the abdomen showing (A) empty right adrenal and renal fossa and (B, C) metastasis seen in the vertebrae.
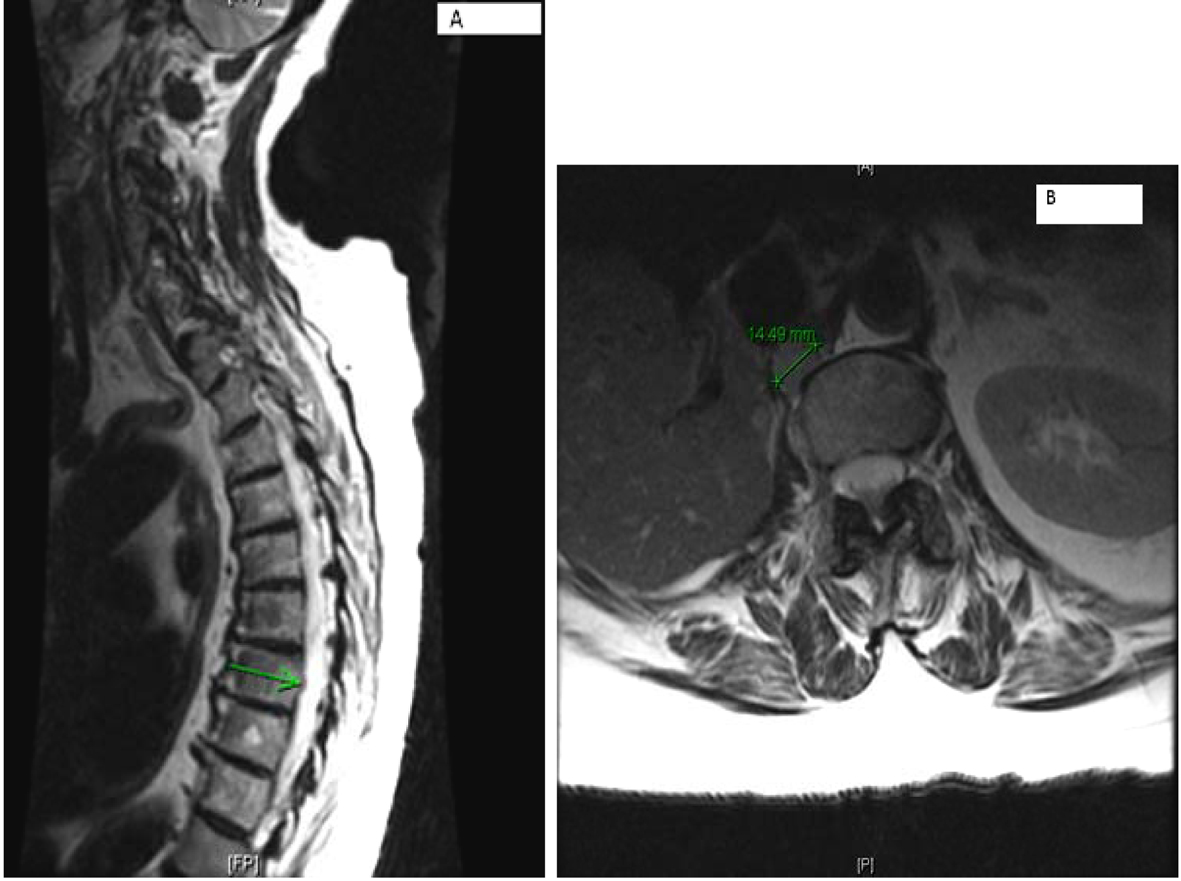
Figure 4. (A) Multilevel-multifocal osseous metastases particularly within thoracolumbar spine with slight epidural extension at T-7 and mild epidural disease at T-10 without cord compression. (B) Right retrocrural/paraspinal metastasis is seen at T-12 and L-1 level measuring about 1.5 cm.
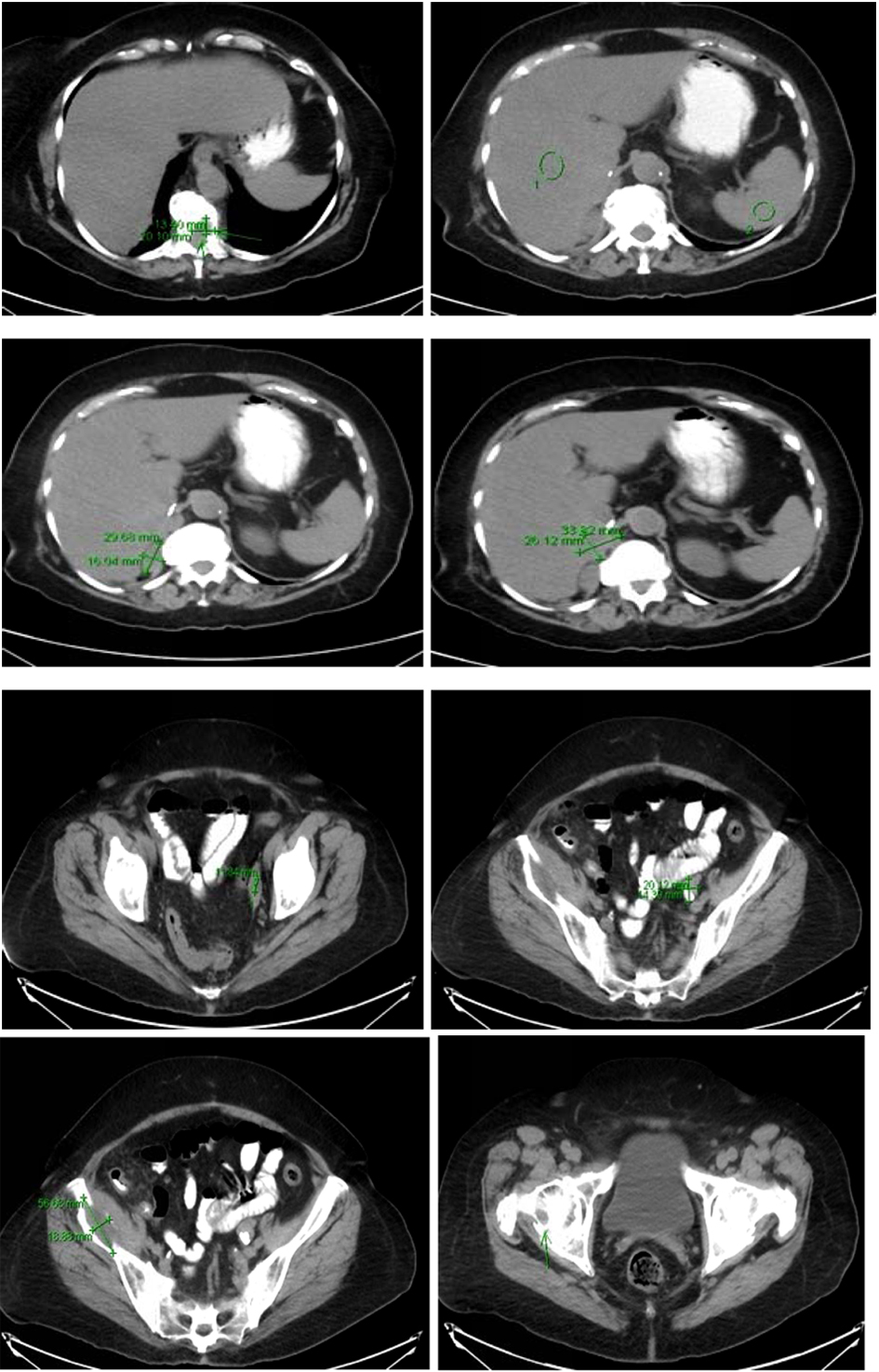
Figure 5. Multiple predominantly osseous metastasis with metastasis in the right iliac bone, increased conspicuity of several soft tissue nodules in the right adrenalectomy bed consistent with recurrent neoplasm, a superior structure measuring 3.4 × 2.6 cm not well defined from adjacent unopacified liver is seen, the right diaphragmatic crus and the unopacified IVC and an adjacent posterior nodule measuring 3 × 1.6 cm is noted.
Table
Table 1. Pheochromocytoma of the Adrenal Gland Scoring Scale (PASS)
| Nuclear hyperchromasia | 1 |
| Profound nuclear pleomorphism | 1 |
| Capsule invasion | 1 |
| Vascular invasion | 1 |
| Extension into adipose tissue | 2 |
| Atypical mitotic figures | 2 |
| Greater than 3 of 10 mitotic figures high-power field | 2 |
| Tumor cell spindling | 2 |
| Cellular monotony | 2 |
| High cellularity | 2 |
| Central or confluent tumor necrosis | 2 |
| Large nests or diffuse growth (> 10% of tumor volume) | 2 |
| Total | 20 |