World Journal of Oncology, ISSN 1920-4531 print, 1920-454X online, Open Access
Article copyright, the authors; Journal compilation copyright, World J Oncol and Elmer Press Inc
Journal website http://www.wjon.org
Case Report
Volume 8, Number 4, August 2017, pages 122-125
Rare Case of Spinal Cord Compression as Initial Presentation of Thymic Carcinoma
Prabhsimranjot Singha, e, Ankur Sinhab, Sonali Malhotrac, Abhinav Binod Chandrad, William Solomona, Yiwu Huanga
aDepartment of Hematology/Oncology, Maimonides Cancer Center, Brooklyn, New York, USA bDepartment of Internal Medicine, Maimonides Medical Center, Brooklyn, New York, USA cDepartment of Pediatric Endocrinology, Infant and Children’s Hospital of Brooklyn, Maimonides Medical Center, Brooklyn, New York, USA dDepartment of Hematology Oncology, Yuma Regional Medical Center Yuma, Arizona, USA eCorresponding Author: Prabhsimranjot Singh, Department of Hematology/Oncology, Maimonides Medical Center, 4802 10th Avenue, Brooklyn, NY 11219, USA
Manuscript submitted June 22, 2017, accepted July 4, 2017 Short title: Thymic Carcinoma With Spinal Cord Compression doi: https://doi.org/10.14740/wjon1053w
Thymic carcinomas are rare aggressive cancers with limited clinical trial data. Its usual treatment is surgical resection with variable response to chemotherapy and radiation. It usually presents as anterior mediastinal mass with late sequela of metastases to the lymph nodes, pleura and bones. We present of thymic carcinoma with a rare initial presentation of vertebral metastases causing spinal cord compression.
Keywords: Thymic carcinoma; Spinal cord compression; Anterior mediastinal mass
Thymic carcinoma has been well recognized as an aggressive malignancy. It has distinct features that differentiate it from a thymoma. These include atypia on cytology, and a propensity to metastasize. Several reports have documented loco-regional metastases to the pleura, diaphragm and the pericardium as well as rare extra-thoracic metastases. Involvement of the spine with cord compression leading to neurological compromise is very rare. We present our experience treating a patient with thymic carcinoma who presented with back pain as the only initial complaint.
A 29-year-old male patient with no past medical problems presented with 2-week history of progressively worsening back pain. He reported to have back pain for the past 3 months, but recently noticed that pain became more severe, with radiation to the left leg making ambulation difficult. He denied any bowel or urinary incontinence. At the time of initial presentation, neurological examination revealed equal and adequate strength in all extremities, but no gross sensory loss. A prominent non-tender left supraclavicular lymphadenopathy was palpated and scrotal fullness without any definitive testicular mass was appreciated. Laboratory evaluation demonstrated hemoglobin of 10.5 g/dL, white cell count of 130,000/UL with mostly neutrophils, lactic acid dehydrogenase of 528 IU/L, alpfa fetoprotein of 1.1 ng/mL and beta human chorionic gonadotrophin of 1.0 mIU/mL. Serum protein and urine electrophoresis did not detect a monoclonal protein.
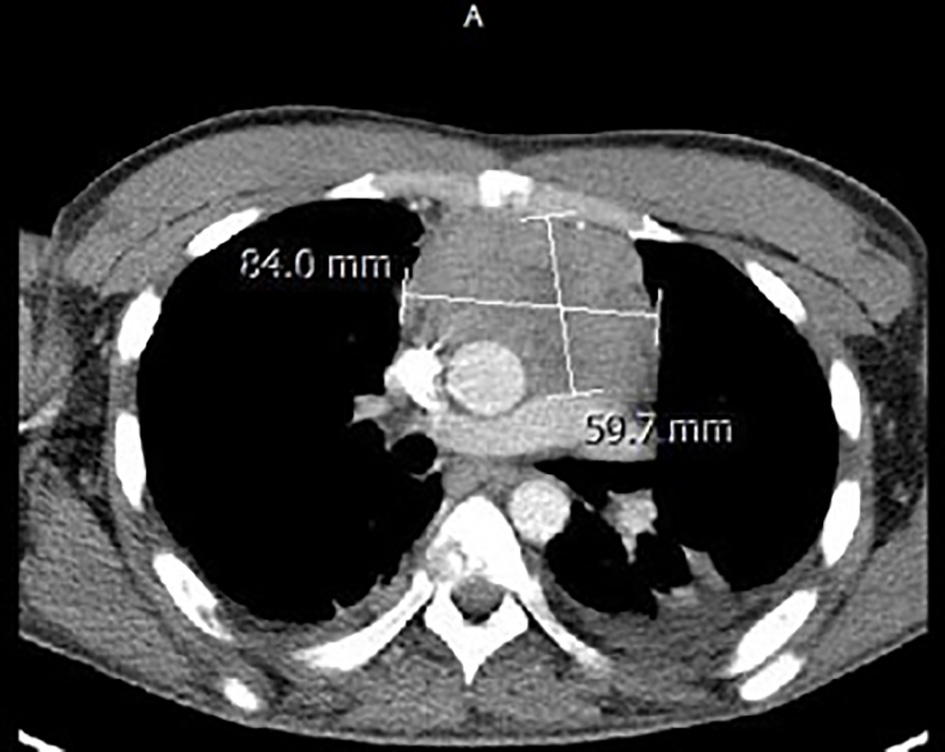
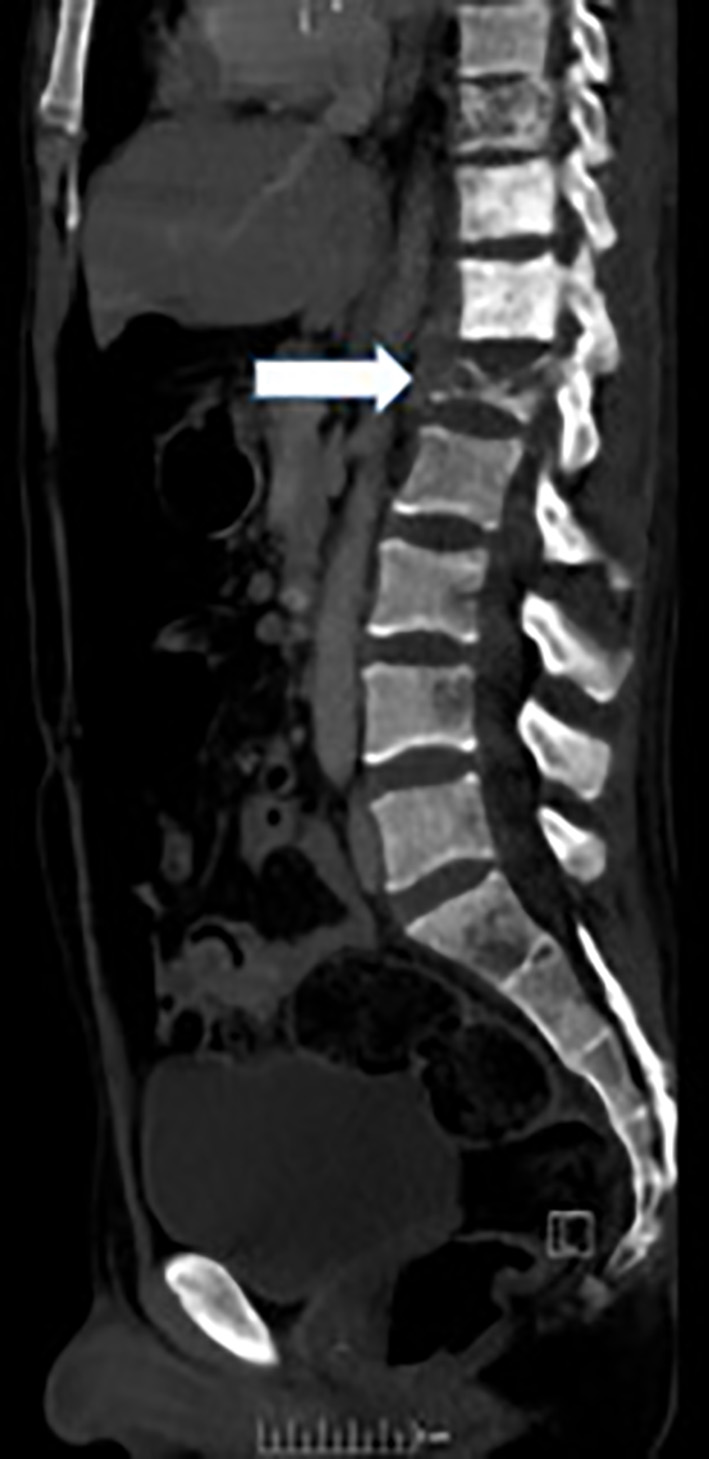
Magnetic resonance imaging (MRI) of the spine reported an epidural mass at T12-L1 level with spinal canal stenosis at T12 level (Fig. 1). Further workup included CT of chest/abdomen and pelvis which showed a large anterior mediastinal mass measuring 8.4 × 5.9 cm (Fig. 2), mixed lytic/sclerotic bony lesions in the spinal bodies from T10 to L1 (Fig. 3), the iliac crests, left sacrum, and the left ischial tuberosity and left supraclavicular lymphadenopathy (Fig. 4). The differential at that time inclined towards germ cell tumor and lymphoma and decision was made to biopsy the left supraclavicular fossa lymph node.
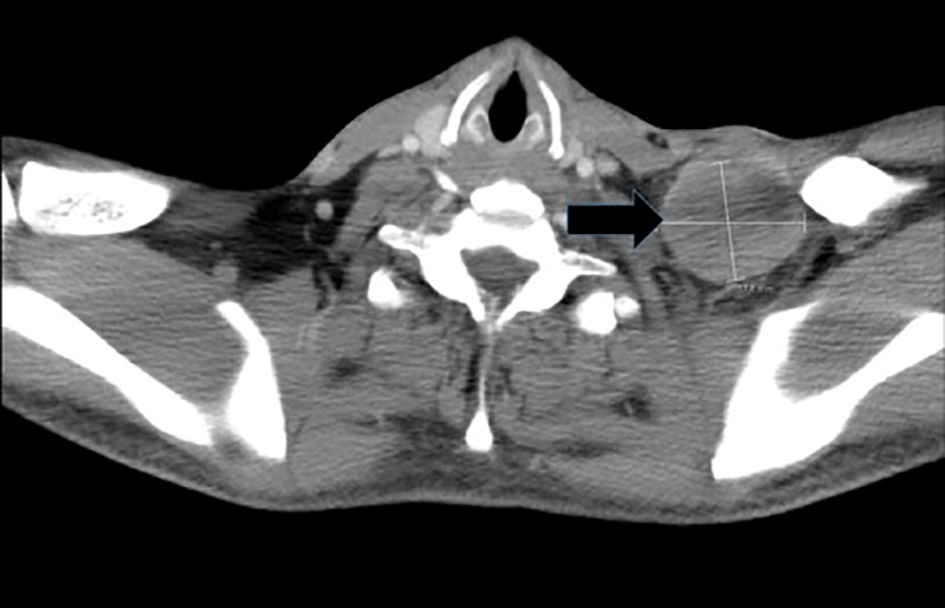
Figure 4. CT image depicting left supraclavicular lymphadenopathy/mass.
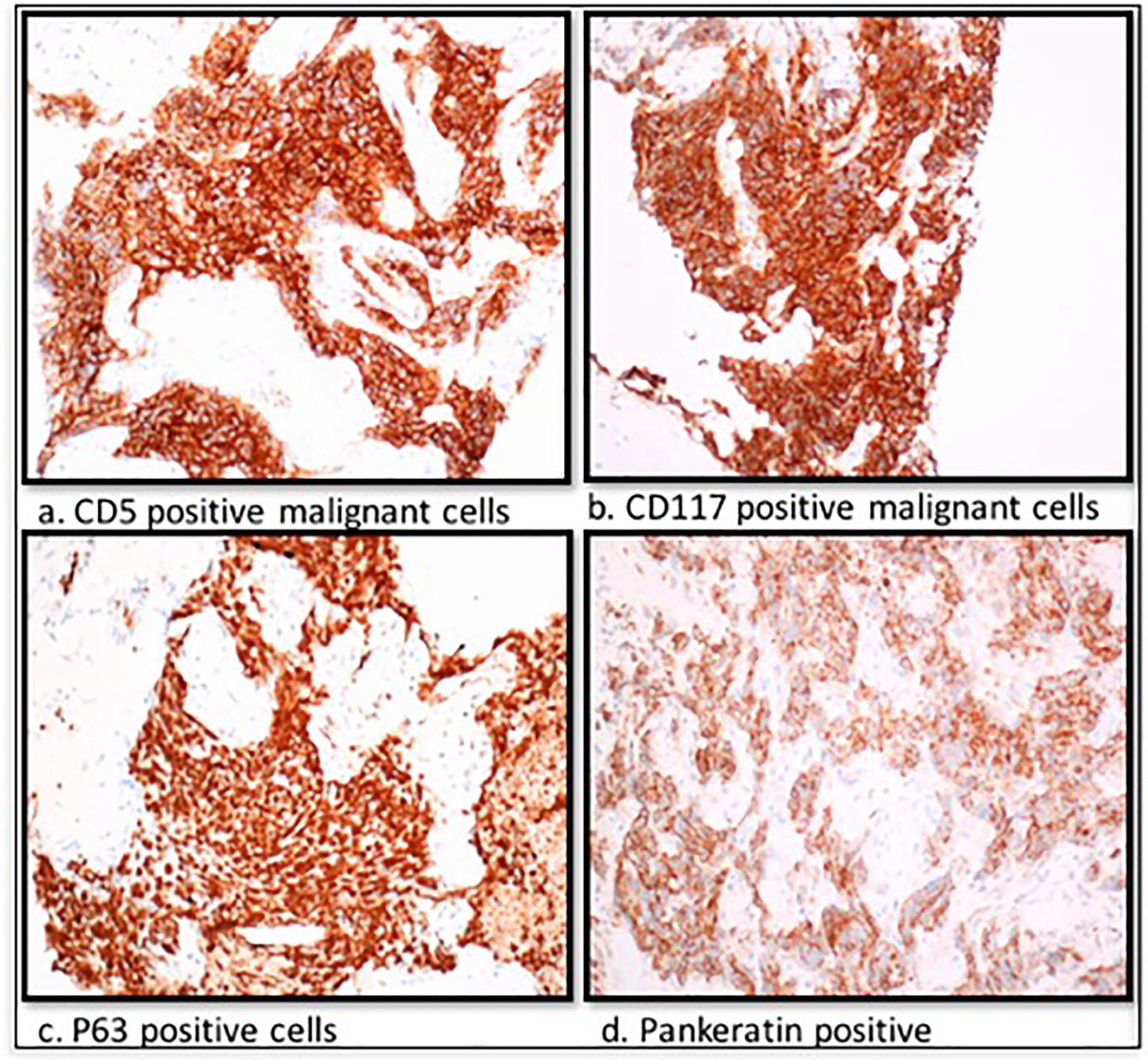
Histopathological analysis of the biopsy revealed positive immunohistochemical markers AE1 and AE3, CD5, CD117, P63 and pankeratin (Fig. 5) and negative CD45, CD 117 and CD20 consistent with diagnosis of primary thymic carcinoma. On day 5 of admission, there was a worsening of muscle power in the lower extremities with 4/5 in right and 3/5 in left lower extremity, respectively. Neurosurgical intervention with a T11-L1 laminectomy and resection of epidural tumor was performed. Surgical pathology of the T12 epidural mass was similar to the left supraclavicular node biopsy formulating a final diagnosis of metastatic thymic carcinoma with a rare initial presentation with spinal cord compression.
Subsequently, patient was treated with palliative radiation and chemotherapy with carboplatin and paclitaxel along with denosumab with some symptom relief. Unfortunately, after two cycles of chemotherapy, he had evidence of disease progression with a CT scan reporting enlarging anterior mediastinal mass and new lymphadenopathy and multiple bone lesions. A bone scan showed multiple bone lesions and was subsequently treated with palliative radiation to the left hip and distal femur for pain control. The patient and his family decided to receive palliative care and went to home hospice where our patient passed away approximately 6 months from his initial presentation.
Thymic carcinoma is a rare neoplasm with about 0.06% constitution amongst all thymic tumors [1]. Levine and Rosai [2] initially classified thymic carcinoma into five types, and this classification was simplified into two groups by Rosai and Suster, namely “high grade” and “low grade” based on histology [3]. Masaoka et al proposed a staging system for thymic carcinoma that considered local as well as regional spread for staging [4]. This is known as the Masaoka-Koga staging system and our patient was stage IVB, due to distant extra-thoracic metastases present on diagnosis. The histological grade as well as the stage at presentation plays a pivotal role in prognosis as well as further management of the disease. A study reported a 5-year survival of 15-20% for high grade thymic carcinomas [5].
Thymic carcinoma metastasizes to distant organs mainly the liver, kidney and bones [6]. Literature search revealed that spinal metastases are extremely rare, a case series reported seven cases of spinal metastases at a single center, but none of these cases presented with back pain and cord compression as the initial presenting symptom [7]. Spinal lesions were late sequelae of the disease and represented poor prognosis [7].
A lack of randomized case-control studies comparing treatment modalities has led to a paucity of clinical guidelines for treatment. Surgical management with complete resection of the thymic carcinoma remains the primary modality of treatment [8] with possible neoadjuvant radiotherapy aimed at tumor shrinkage, thereby aiding surgery. Myojin et al reported that preoperative radiotherapy could aid in tumor shrinkage and improve survival for patients with locally advanced tumor [9]. Nonaka et al reported significantly better outcomes in patients who received postoperative radiotherapy with low rate of recurrence in patients who received mediastinal irradiation [10]. Our patient had distant metastases at presentation, and he underwent spinal cord decompression followed by radiation to spine. He regained power to his lower extremities post-surgery and improvement in his quality of life.
Platinum-based chemotherapy plays an important role in management of advanced thymic carcinomas. Yoh et al compared the outcomes of four platinum-based chemotherapy regimens and concluded that 46% of the patients had an objective response to this therapy [11]. Given the moderate response to chemotherapy, new modalities for treatment need to be developed. Sorafenib and sunitinib are oral multikinase inhibitors which have shown anti-tumor activity in chemotherapy refractory thymic carcinomas that express c-kit (CD-117) and VEGF [12-14]. Another drug belinostat, which is a histone deacetylase (HDAC) inhibitor, has shown some promise. The HDAC inhibitors work by regulating expression of tumor suppressor genes by altering DNA and chromatin [15]. Our patient had rapid progression of his disease with deterioration of performance status and succumbed to the illness despite radiation as well as chemotherapy.
To conclude we would like to stress on the importance of timely diagnosis as well as urgent surgical planning to achieve complete resection. This should be accompanied with a multimodality approach involving neoadjuvant as well as postoperative chemotherapy and/or radiotherapy.
Levine GD, Rosai J. Thymic hyperplasia and neoplasia: a review of current concepts. Hum Pathol. 1978;9(5):495-515. doi
Suster S, Rosai J. Thymic carcinoma. A clinicopathologic study of 60 cases. Cancer. 1991;67(4):1025-1032. doi
Masaoka A, Monden Y, Nakahara K, Tanioka T. Follow-up study of thymomas with special reference to their clinical stages. Cancer. 1981;48(11):2485-2492. doi
Strollo DC, Rosado-de-Christenson ML, Jett JR. Primary mediastinal tumors: part II. Tumors of the middle and posterior mediastinum. Chest. 1997;112(5):1344-1357. doi
Jee TK, Lee SH, Kim HJ, Kim ES, Eoh W. Spinal metastasis of thymic carcinoma as a rare manifestation: a summary of 7 consecutive cases. Korean J Spine. 2014;11(3):157-161. doipubmed
McKenna WG, Bonomi P, Barnes MM, Glatstein E. Malignancies of the thymus. In: Roth JA, Ruckdeschel JC, Weisenburger TH, editors. Thoracic Oncology. Philadelphia (PA): W.B. Saunders, Co. 1989; p. 466-477.
Myojin M, Choi NC, Wright CD, Wain JC, Harris N, Hug EB, Mathisen DJ, et al. Stage III thymoma: pattern of failure after surgery and postoperative radiotherapy and its implication for future study. Int J Radiat Oncol Biol Phys. 2000;46(4):927-933. doi
Nonaka T, Tamaki Y, Higuchi K, Katoh H, Nakahashi M, Horikoshi H, Takahashi K, et al. The role of radiotherapy for thymic carcinoma. Jpn J Clin Oncol. 2004;34(12):722-726. doipubmed
Yoh K, Goto K, Ishii G, Niho S, Ohmatsu H, Kubota K, Kakinuma R, et al. Weekly chemotherapy with cisplatin, vincristine, doxorubicin, and etoposide is an effective treatment for advanced thymic carcinoma. Cancer. 2003;98(5):926-931. doipubmed
Li XF, Chen Q, Huang WX, Ye YB. Response to sorafenib in cisplatin-resistant thymic carcinoma: a case report. Med Oncol. 2009;26(2):157-160. doipubmed
Bisagni G, Rossi G, Cavazza A, Sartori G, Gardini G, Boni C. Long lasting response to the multikinase inhibitor bay 43-9006 (Sorafenib) in a heavily pretreated metastatic thymic carcinoma. J Thorac Oncol. 2009;4(6):773-775. doipubmed
Thomas A, Rajan A, Berman A, Tomita Y, Brzezniak C, Lee MJ, Lee S, et al. Sunitinib in patients with chemotherapy-refractory thymoma and thymic carcinoma: an open-label phase 2 trial. Lancet Oncol. 2015;16(2):177-186. doi
Bertrand P. Inside HDAC with HDAC inhibitors. Eur J Med Chem. 2010;45(6):2095-2116. doipubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Oncology is published by Elmer Press Inc.