

| World Journal of Oncology, ISSN 1920-4531 print, 1920-454X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Oncol and Elmer Press Inc |
| Journal website https://www.wjon.org |
Letter to the Editor
Volume 13, Number 3, June 2022, pages 155-158

Radiation Therapy for Prostate Cancer: Challenges Facing Low-Middle Income Countries During COVID Pandemic
Ramiz Abu-Hijliha, c, Fawzi Abuhijlaa, Issa Mohamada, Mohammed Shahaitb
aRadiation Oncology Department, King Hussein Cancer Center, Amman 11941, Jordan
bSurgical Oncology Department, King Hussein Cancer Center, Amman 11941, Jordan
cCorresponding Author: Ramiz Abu-Hijlih, King Hussein Cancer Center, Amman 11941, Jordan
Manuscript submitted April 6, 2022, accepted May 23, 2022, published online June 2, 2022
Short title: RT for PC: Challenges in LMICs During COVID
doi: https://doi.org/10.14740/wjon1484
| To the Editor | ▴Top |
Since the emergence of coronavirus disease 2019 (COVID-19) pandemic, cancer care has been adjusted to adapt with overloaded hospitals and healthcare staff shortage. Radiation therapy (RT) is considered one of the cornerstone modalities of prostate cancer management. Response to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection varied between developing countries according to the infection rate, healthcare infrastructure and technologic capabilities in RT units. As such, active surveillance in early-stage disease, delay of RT treatment and use of shorter RT courses have been implemented as a short-term solution. COVID-19 vaccines have been available for a year time. Unfortunately, developing countries were obliged to wait for developed countries to complete their vaccination rollout. In this editorial, we highlight prostate cancer management challenges during COVID-19 pandemic in low-middle income countries (LMICs) from radiation oncology perspective.
Prostate cancer is the second most common cancer among men worldwide. While the incidence rate is the highest in Europe, North America, and Australia, Asia has the lowest incidence rate [1]. In Jordan, 451 new cases were expected in 2020 according to Global Cancer Incidence, Mortality and Prevalence (GLOBOCAN) report, with age-standardized incidence rate of 15.8 per 100,000 vs. 30.7 worldwide and 83.4 in Northern Europe [2]. Nevertheless, the ratio of mortality to incidence in Jordan is double the ratio in western countries (0.33 vs. 0.17), which can be attributable to substantial number of patients present with metastatic disease at time of initial diagnosis in the Middle East region [3].
In early 2020, the SARS-CoV-2 infection was announced as a pandemic [4]. During the pandemic, hospitals worldwide were suffering from increased number of COVID-19 patients and lack of medical supplies. Elective procedures were canceled because hospitals were occupied with surge of COVID-19 patients. Cancer care was not an exception and many interventions were canceled or postponed as well [5].
The COVID-19 pandemic was associated financial and social challenges, which were reflected on healthcare systems [5]. LMICs were more affected than rest of the world as their healthcare systems were already facing diverse problems of poor infrastructure, lack of funding, and absence of effective administrative and strategic planning [6]. RT is one of the main treatments for prostate cancer. More than half of men receive RT during their disease course, either as definitive radical treatment, adjuvant, or palliative intent [3, 6]. However, the access for radiation services depends on availability of RT facilities, financial coverage, and level of expertise available (for instance, more than 90% of residents do not have access to RT treatment in LMICs). Definitely, this has contributed to long waiting time for RT treatment and adoption of old-fashioned RT techniques i.e., two- and three-dimensional conformal RT [6]. To compound the situation, COVID restrictions added to the complexity of the RT availability as a treatment option for patients in LMICs.
For developing countries, the pandemic formed an unprecedented pressure on their resources, especially in war-torn countries and others who received waves of refugees. The same countries were suffering financial restrictions and poor technologic tools when compared with developed countries. Over the past 2 years, there was the gap increased owing to the pandemic [7, 8].
Since the emergence of COVID-19 pandemic, several international bodies issued guidelines helping the physicians to balance between infection control and patient treatment [8]. These guidelines have encouraged the use of more novel treatment schemes and patient flow pathways. For example, virtual clinics, online access to RT planning, and use of hypofractionated regimens are best examples of these measures. Figure 1 illustrates the modified RADS framework which was adapted for management of prostate cancer through the pandemic [9]. Accordingly, management scheme for prostate cancer patients constituted of the following: for very low, low, and favor intermediate risks, treatment can be deferred until pandemic wave subsides. However, unfavorable intermediate and high risks may commence on hormones and RT delivered when infection is controlled. Short radiation schemes such as 60 Gy over 20 fractions in 4 weeks, and stereotactic body radiation (SBRT) as 36.25 Gy over five fractions are always encouraged.
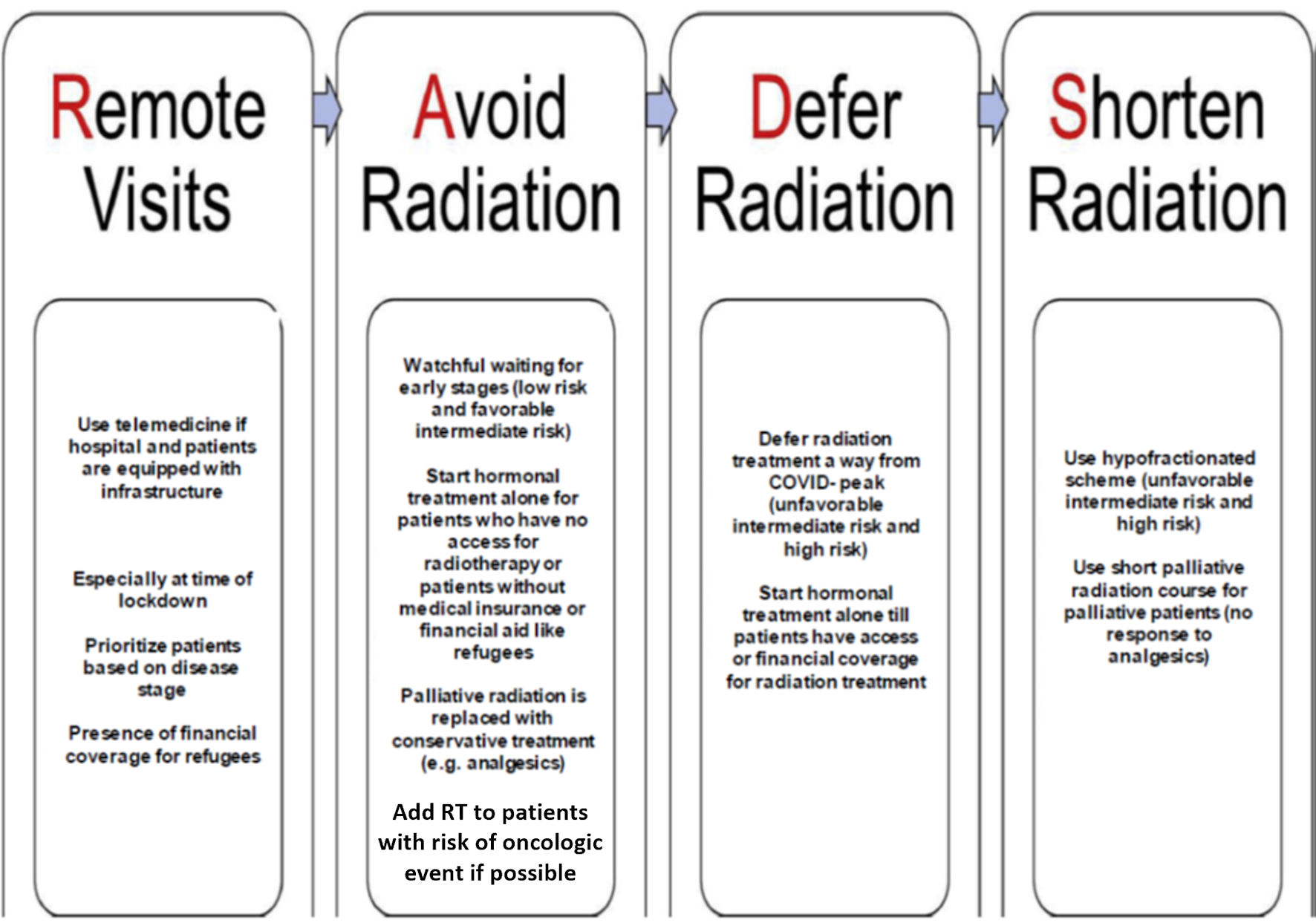 Click for large image | Figure 1. Modified RADS framework for developing countries. RT: radiation therapy; COVID: coronavirus disease. |
Radiation treatment for prostate cancer can be delivered by external beam radiotherapy (EBRT) or brachytherapy. Unfortunately, access to brachytherapy is limited in LMICs because of the cost and high-level training required for the procedure [10]. Aforementioned, for EBRT, hypofractionated regimen is recommended by American Society of Clinical Oncology (ASCO)/American Society for Radiation Oncology (ASTRO)/American Urological Association (AUA) consensus [11], as patients can complete their course in approximately half of the treatment time. However, the access to image-guided technique is limited in LMICs, which might hinder the efforts to adapt these recommendations. On the other hand, online contouring and planning provide an alternative way to perform radiation procedures safely with decrease in infection rate between medical personnel, especially in institutions with advanced infrastructure [12].
Cost-effective studies are paramount at the time of pandemic in developing countries. The ProtecT trial by Hamdy et al found no survival advantage of RT treatment compared to watchful waiting and surgery in low and intermediate risk prostate cancer, although the risk of distant metastases in active treatment arms was approximately half the risk in patients on active surveillance [13]. So those patients can be safely followed during the pandemic and the limited resources can be directed towards more exigent medical necessity.
Vaccines wrote a new chapter. With the introduction of COVID-19 vaccines, the number of infections was expected to decrease. Nevertheless, SARS-CoV-2 variants have made the course of the pandemic unpredictable, in particular Omicron (B.1.1.529) which caused unprecedented increase in number of cases worldwide [14]. Moreover, vaccination levels in LMICs countries were much less than developed and rich countries. The unequal access will further slow the recovery in developing countries and add to the current challenges [15].
Prostate cancer patients in LMICs have limited access to RT, which is related to financial obstacles and lack of highly trained personnel. Amid COVID-19 pandemic, the developing countries faced an unexpected strain on their health care system, which is already strained with limited resources and refugees’ problem. Avoid, defer, or replace radiation treatment was employed over the past 2 years in developing countries based on the pandemic situation in each country.
International support is paramount to help LMICs financially and strategically during the pandemic. Providing strong technical infrastructure will help radiation department implement online procedures, which decrease infection spread.
Early administration of COVID-19 vaccine to medical staffs and cancer patients proved to decease symptoms and mortality [16]. Equal distribution of the vaccine will support recovery in developing countries and restore patients’ treatment to previous standard.
Finally, we propose a dynamic management scheme of prostate cancer patients referred for RT in LMICs. This scheme emphasizes on applying suggested measures at time of SARS-CoV-2 infection peak (Fig. 2).
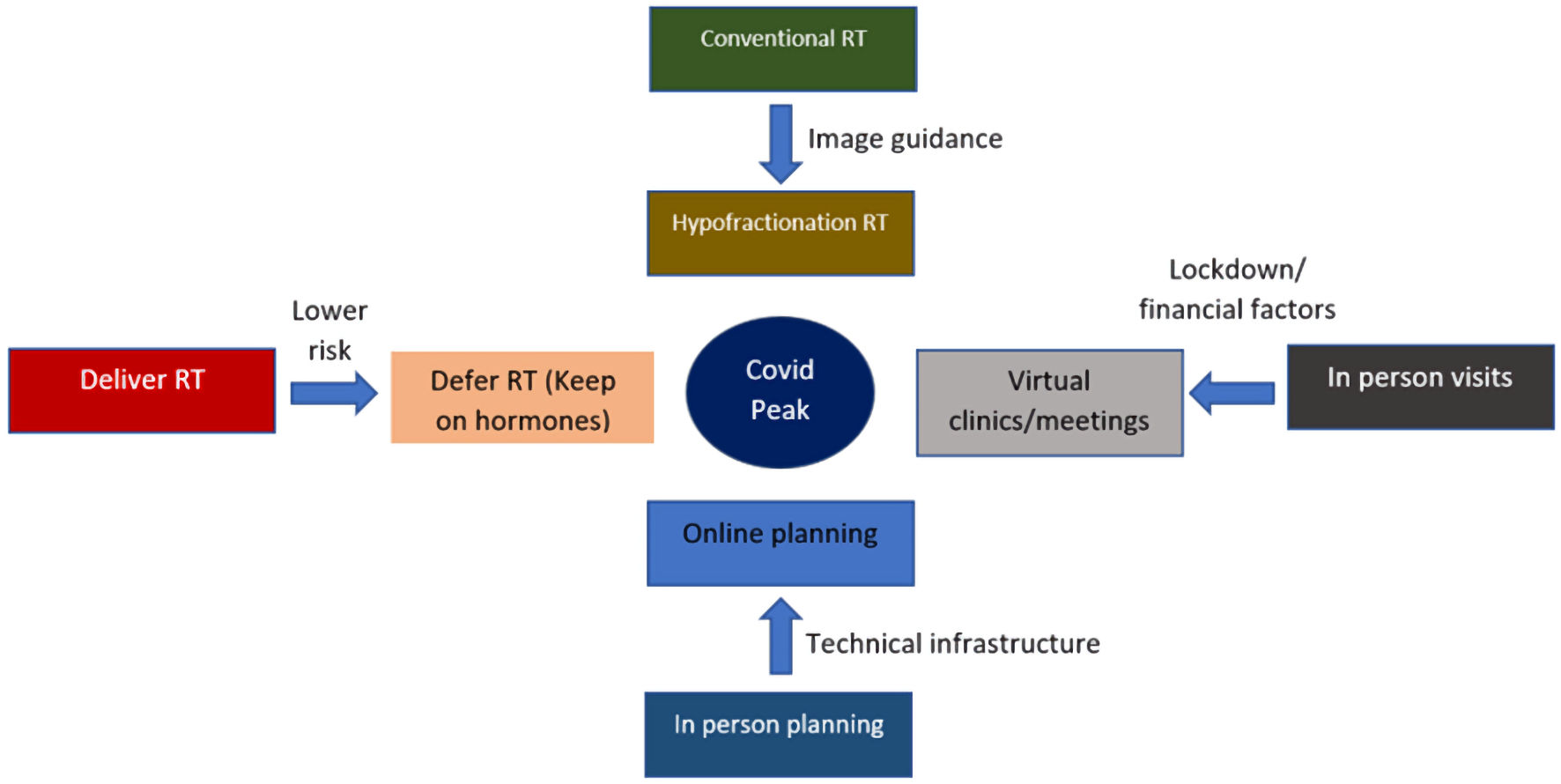 Click for large image | Figure 2. Radiation treatment recommendations according to pandemic situation in middle and low-income country. RT: radiation therapy; COVID: coronavirus disease. |
Acknowledgments
None to declare.
Financial Disclosure
This research did not receive any specific grant from funding agencies in the public, commercial, or any sectors.
Conflict of Interest
All authors declare no conflict of interest, of any kind, related to this work.
Informed Consent
Not applicable.
Author Contributions
All authors have participated in this manuscript. RAH contributed to idea development, writing, and reviewing. FA contributed to writing and editing. IM contributed to editing and reviewing. MS contributed to writing and reviewing.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424.
doi pubmed - Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-249.
doi pubmed - Hilal L, Shahait M, Mukherji D, Charafeddine M, Farhat Z, Temraz S, Khauli R, et al. Prostate cancer in the Arab world: a view from the inside. Clin Genitourin Cancer. 2015;13(6):505-511.
doi pubmed - Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020;91(1):157-160.
- Alhalaseh YN, Elshabrawy HA, Erashdi M, Shahait M, Abu-Humdan AM, Al-Hussaini M. Allocation of the "Already" limited medical resources amid the COVID-19 pandemic, an iterative ethical encounter including suggested solutions from a real life encounter. Front Med (Lausanne). 2020;7:616277.
doi pubmed - Zubizarreta EH, Fidarova E, Healy B, Rosenblatt E. Need for radiotherapy in low and middle income countries - the silent crisis continues. Clin Oncol (R Coll Radiol). 2015;27(2):107-114.
doi pubmed - Ghazinoory S, Majidi B, Nasri S, Zandi ME, Farrokhi H, Javedani M, Barzanouni M. Differences between health technology assessment topics in high- and middle-income countries: a scoping review. Arch Public Health. 2021;79(1):225.
doi pubmed - Mired D, Johnson S, Tamamyan G. Cancer disparities in war-torn and post-war regions. Nat Rev Cancer. 2020;20(7):359-360.
doi pubmed - Zaorsky NG, Yu JB, McBride SM, Dess RT, Jackson WC, Mahal BA, Chen R, et al. Prostate cancer radiation therapy recommendations in response to COVID-19. Adv Radiat Oncol. 2020;5(4):659-665.
doi pubmed - Grover S, Longo J, Einck J, Puri P, Brown D, Chino J, Mahantshetty U, et al. The unique issues with brachytherapy in low- and middle-income countries. Semin Radiat Oncol. 2017;27(2):136-142.
doi pubmed - Morgan SC, Hoffman K, Loblaw DA, Buyyounouski MK, Patton C, Barocas D, Bentzen S, et al. Hypofractionated radiation therapy for localized prostate cancer: executive summary of an ASTRO, ASCO, and AUA evidence-based guideline. Pract Radiat Oncol. 2018;8(6):354-360.
doi pubmed - Siavashpour Z, Goharpey N, Mobasheri M. Radiotherapy based management during Covid-19 pandemic - A systematic review of presented consensus and guidelines. Crit Rev Oncol Hematol. 2021;164:103402.
doi pubmed - Hamdy FC, Donovan JL, Lane JA, Mason M, Metcalfe C, Holding P, Davis M, et al. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med. 2016;375(15):1415-1424.
doi pubmed - Meo SA, Meo AS, Al-Jassir FF, Klonoff DC. Omicron SARS-CoV-2 new variant: global prevalence and biological and clinical characteristics. Eur Rev Med Pharmacol Sci. 2021;25(24):8012-8018.
- Sawal I, Ahmad S, Tariq W, Tahir MJ, Essar MY, Ahmed A. Unequal distribution of COVID-19 vaccine: A looming crisis. J Med Virol. 2021;93(9):5228-5230.
doi pubmed - Lamptey E. Post-vaccination COVID-19 deaths: a review of available evidence and recommendations for the global population. Clin Exp Vaccine Res. 2021;10(3):264-275.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Oncology is published by Elmer Press Inc.