

| World Journal of Oncology, ISSN 1920-4531 print, 1920-454X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Oncol and Elmer Press Inc |
| Journal website http://www.wjon.org |
Case Report
Volume 1, Number 6, December 2010, pages 250-251
Post-Irradiation Morphea in Breast Cancer: An Uncommon Differential Diagnosis to Keep in Mind
Francisco Javier Afonso-Afonsoa, d, Maria Pilar Arevalob, Fernando Campo Cerecedoc, Laura De Paz Ariasa, Cristina Durana Tonderc
aMedical Oncology Section, Complejo Hosp. A. Marcide, Ferrol, A Coruna, Spain
bDermatology Service, Complejo Hosp. A Coruna, A Coruna, Spain
cPathology Service, Complejo Hosp. A. Marcide, Ferrol, A Coruna, Spain
dCorresponding author: Complejo Hosp. A. Marcide, Ctra Gral de Catabois S/N. 15405- Ferrol, A Coruna, Spain
Manuscript accepted for publication December 16, 2010
Short title: Post-Irradiation Morphea in Breast Cancer
doi: https://doi.org/10.4021/wjon264w
| Abstract | ▴Top |
Breast cancer is the most common cancer in women of developed countries. Early stage diagnosis is followed, in many cases, of conservative surgery and local radiotherapy. This treatment reduces loco-regional recurrences but may be accompanied by local complications. Morphea of the breast is an uncommon skin condition and has been described after radiotherapy. The inflammatory stage of morphea can commonly be mistaken for a local recurrence or inflammation. We report the case of a 51-year-old woman with breast cancer who underwent a conservative surgery with postoperative chemo and radiotherapy. She developed a sclerodermiform plaque with a biopsy that showed histopathological changes consistent with morphea.
Keywords: Morphea; Breast cancer; Radiotherapy
| Introduction | ▴Top |
Morphea is a localized scleroderma variety that can be divided into localized (circumscribed) or generalized disease, and is characterized by patches of sclerotic skin that develop on the trunk and limbs at sites of previously normal texture, preferably in the trunk of women of medium age. During the last decade, some cases of radiotherapy related morphea has been reported in breast cancer patients, with great clinical similarity between this entity and a local recurrence. Thus, it is a very important issue to keep in mind this idiopathic disease in the differential diagnosis of a breast cancer patient with a probably local post-radiotherapy recurrence.
| Case Report | ▴Top |
A 51-year-old post-menopause Caucasian woman was diagnosed with right breast carcinoma. Histopathological diagnosis was made from a needle biopsy: invasive ductal adenocarcinoma, with positivity for estrogen and progesterone receptors and negative C-erbB2. A wide local excision of the right breast and axillary node sampling was realized and post operatory histology identified a T1N1 grade 2 invasive ductal carcinoma without margins invasion. She was treated with adjuvant chemotherapy using four cycles of doxorubicin and ciclofosfamide followed by four cycles of docetaxel. Letrozole 2.5 mg every day was taken when chemotherapy was concluded and conventional external radiotherapy to the right breast, axillary and internal mammary nodes were indicated, with a total dose of 50 Gy. Eleven months after the radiotherapy end, patient developed a pruritic plaque of gradual growth located in the radiotherapy field on the right breast. Mammography and ultrasound scan demonstrated a thickness of the cellular subcutaneous tissue and a density increase of the underlying fat. Office inspection showed an irregular indurate plaque, with irregular borders and “a peau d´orange” aspect. A biopsy revealed non epidermis changes and dermis thickness with numerous thick of collagen fibers that in depth were penetrating into the fatty lobules of the cellular subcutaneous tissue, a slight inflammatory infiltrate, and an atrophy of pilocebaceous units, consistent with a diagnosis of localized scleroderrmia (morphea) (Fig. 1). Patient was treated with topical local steroids, with progressive improvement and without new loco-regional dermatological events.
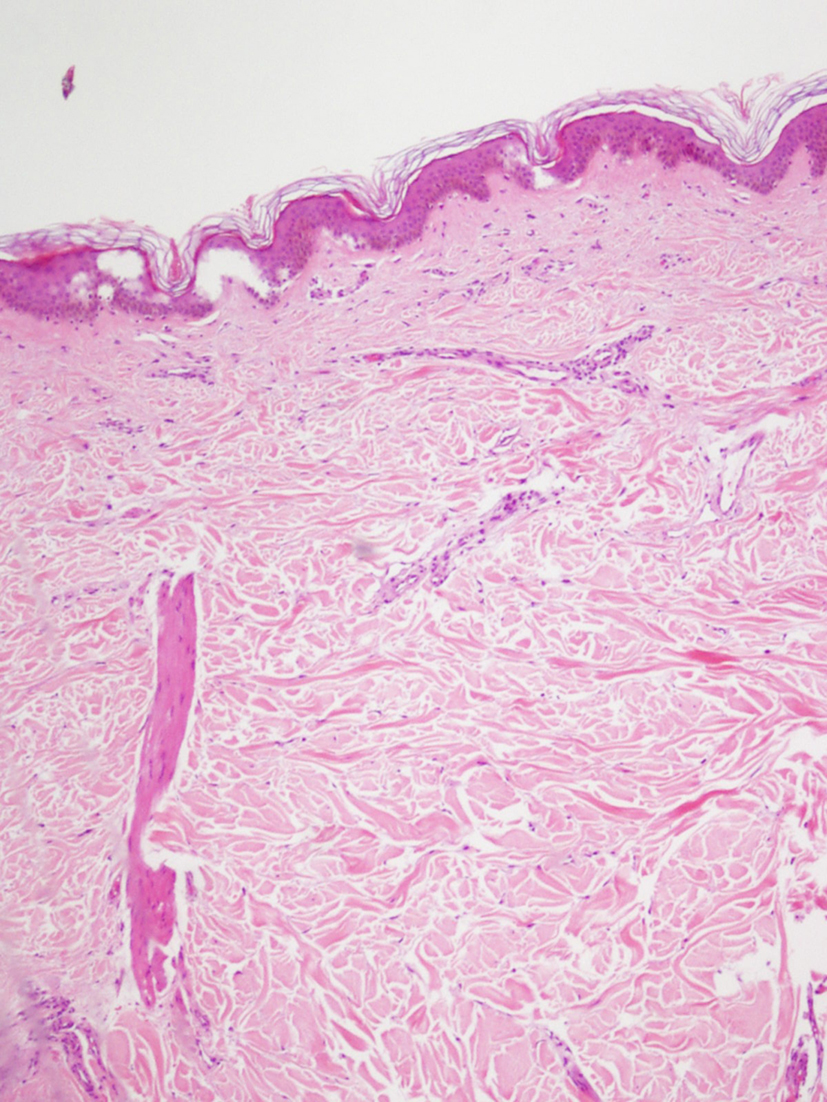 Click for large image | Figure 1. Dermis with numerous thickened collagen fibers parallel to the basal layer and atrophy of skin appendages (HE x 100). |
| Discussion | ▴Top |
In developed countries, breast cancer is the most frequent neoplasm in women. Conservative surgery, followed by local radiotherapy is a common modality used in the treatment of this disease. This treatment reduces loco-regional recurrences but may be accompanied by local acute (erythema and desquamation) or chronic fibrosis (10%), skin telangiectasia (10%), atrophy (8%), and pain (2%) [1]. Morphea is a localized scleroderma variety that can be divided into localized (circumscribed) or generalized disease, and is characterized by patches of sclerotic skin that develop on the trunk and limbs at sites of previously normal texture, preferably in the trunk of women of medium age [2]. Morphea post-radiotherapy is a rare complication, with an estimated incidence of 1 in 500 patients [3], in contrast to that of morphea (of any etiology), which is 2.7 per 100 000 in the general population per year [4], and its onset ranges from 1 to 12 months, but can be as late as 32 years post-radiotherapy [5, 6]. Today, we know that there is no relationship with the total radiotherapy dose [7]. All the involved pathogenic mechanisms are not known, but it is accepted that radiotherapy-induced morphea has an initial inflammatory phase and a subsequent 'burnt-out' phase, where the latter displays induration, fibroid retraction, and pigmentation of the breast. The pathophysiology is thought to be radiation-induced neoantigen formation that subsequently stimulates secretion of transforming growth factor beta (TGF-β). TGF-β strongly induces fibroblast activation, collagen synthesis, and, hence, excessive fibrosis [5, 6]. Usually, the clinical course of radiotherapy-induced morphea is benign and it will usually improve with any of the many treatments that have been used with varying results, including oral and topical antibiotics, intralesional or systemic steroids, oral antimalarial drugs, or phototherapy [5]. Some publications suggest that radiotherapy alone most likely is not sufficient to provoke morphea and surgery is an important but as yet underestimated risk factor in disease etiogenesis [8]. Hence, probably a synergistic pathogenic effect of both treatment modalities in a subset of patients with particular immunologic characteristics triggers the manifestation of this entity. During the last decade, some cases of radiotherapy related morphea has been reported in breast cancer patients, with great clinical similarity between this entity and a local recurrence. Thus, it is a very important issue to keep in mind this idiopathic disease in the differential diagnosis of a breast cancer patient with a probably local post-radiotherapy recurrence.
| References | ▴Top |
- Fehlauer F, Tribius S, Holler U, Rades D, Kuhlmey A, Bajrovic A, Alberti W. Long-term radiation sequelae after breast-conserving therapy in women with early-stage breast cancer: an observational study using the LENT-SOMA scoring system. Int J Radiat Oncol Biol Phys. 2003;55(3):651-658.
pubmed doi - Falanga V. Localized scleroderma. Med Clin North Am. 1989;73(5):1143-1156.
pubmed - Bleasel NR, Stapleton KM, Commens C, Ahern VA. Radiation-induced localized scleroderma in breast cancer patients. Australas J Dermatol. 1999;40(2):99-102.
pubmed doi - Ardern-Jones MR, Black MM. Widespread morphoea following radiotherapy for carcinoma of the breast. Clin Exp Dermatol. 2003;28(2):160-162.
pubmed doi - Schaffer JV, Carroll C, Dvoretsky I, Huether MJ, Girardi M. Postirradiation morphea of the breast presentation of two cases and review of the literature. Dermatology. 2000;200(1):67-71.
pubmed doi - Davis DA, Cohen PR, McNeese MD, Duvic M. Localized scleroderma in breast cancer patients treated with supervoltage external beam radiation: radiation port scleroderma. J Am Acad Dermatol. 1996;35(6):923-927.
pubmed doi - Martin JM, Pinazo MI, Monteagudo C, Calduch L, Ramón D, Jordá E. Morfea tras tratamiento radioterápico por cancer de mama. Med Cutan Iber Lat Am. 2003;31(1):38-41.
- Trattner A, Figer A, David M, Lurie H, Sandbank M. Circumscribed scleroderma induced by postlumpectomy radiation therapy. Cancer. 1991;68(10):2131-2133.
doi
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Oncology is published by Elmer Press Inc.