

| World Journal of Oncology, ISSN 1920-4531 print, 1920-454X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Oncol and Elmer Press Inc |
| Journal website https://www.wjon.org |
Original Article
Volume 15, Number 3, June 2024, pages 463-471

Deciphering Trends in Cancer Mortality: A Comprehensive Analysis of Brazilian Data From 1979 to 2021 With Emphasis on Breast and Prostate Cancers
Leonardo Pires Paredesa, Marlon da Silva Brandao Rodriguesa, Ralph Santos-Oliveiraa, b
aBrazilian Nuclear Energy Commission, Nuclear Engineering Institute, Rio de Janeiro 21941906, Brazil
bCorresponding Author: Ralph Santos-Oliveira, Brazilian Nuclear Energy Commission, Nuclear Engineering Institute, Rio de Janeiro 21941906, Brazil
Manuscript submitted January 30, 2024, accepted March 30, 2024, published online April 15, 2024
Short title: Deciphering Trends in Cancer Mortality
doi: https://doi.org/10.14740/wjon1831
| Abstract | ▴Top |
Background: This study examined cancer mortality trends in Brazil from 1979 to 2021, emphasizing breast and prostate cancers.
Methods: Utilizing data from the Brazilian Mortality Information System and the Brazilian Institute of Geography and Statistics, it analyzed cancer deaths nationally and regionally, highlighting gender-specific and regional disparities.
Results: The research finds that cancer death rates have been growing at an average of 12% per year, contrasting with the population growth rate of 2.2%. This trend is more pronounced in the southern and southeastern regions of Brazil. A comparison of cancer mortality rates between Brazil, the USA, and China reveals that while the Brazilian and Chinese rates exhibit slower growth, the US rate shows a continuous decline since the 1990s.
Conclusions: The study adopts a novel approach by focusing on growth rates and employing polynomial interpolation, revealing a deceleration in cancer death growth over the last 15 years across all malignant neoplasms. The study also contextualizes these findings within Brazil’s cancer control policies, tracing the evolution of preventive measures and treatment advancements. It highlights the significant role of the National Cancer Institute and the Unified Health System in implementing effective strategies. The decreasing trend in cancer mortality rates in Brazil, despite population growth, illustrates the effectiveness of comprehensive cancer control and prevention measures, underlining their importance in public health policy.
Keywords: Cancer mortality trends; Breast cancer; Prostate cancer; Public health policy; Mortality information system; Growth rate analysis
| Introduction | ▴Top |
Brazil is recognized as one of the largest and most diversified economies in Latin America, with a gross domestic product (GDP) of $3.147 trillion, ranking it among the top 10 in the world. The country boasts a diverse economic landscape comprising agriculture, manufacturing, and services sectors. Its robust agricultural industry is a significant contributor to the economy, with Brazil being a global leader in the production of various commodities, including coffee, sugar, and soybeans [1, 2]. Moreover, the manufacturing sector plays a crucial role, encompassing industries such as automobiles, steel, and petrochemicals. Brazil’s rich natural resources, including substantial reserves of iron ore and crude oil, have also contributed significantly to its economic growth.
The Brazilian healthcare system, known as the Unified Health System (Sistema Unico de Saude (SUS)), is recognized as one of the largest and most comprehensive public healthcare systems globally [3]. Established in 1988, the SUS is founded on the principles of universality, comprehensiveness, and equity, aiming to provide universal access to healthcare services for all citizens. The SUS operates through a decentralized model, with services delivered through a network of public healthcare facilities, including hospitals, clinics, and community health centers. It encompasses a wide range of services, from preventive care and primary healthcare to specialized and high-complexity medical treatments. Despite its comprehensive coverage, the SUS faces various challenges, including underfunding, regional disparities in access to healthcare, and shortages of medical professionals and essential resources [4, 5]. These challenges often result in long wait times for medical procedures and a strain on the system’s capacity to meet the increasing demands of the population. In this sense, several efforts to improve the healthcare system have been ongoing, with initiatives focused on enhancing primary care services, expanding access to specialized care, and implementing health promotion and disease prevention programs [6, 7].
Cancer remains one of the most significant global public health challenges, with a profound impact on morbidity and mortality worldwide. The World Health Organization (WHO) estimates that cancer is the second leading cause of death globally, responsible for approximately 10 million deaths each year [8].
The burden of cancer varies across different regions and populations, with variations in incidence, prevalence, and mortality rates. In Brazil, cancers have a considerable impact on the country’s healthcare system and population. It is one of the leading causes of morbidity and mortality, contributing to a substantial burden of disease. The most prevalent types of cancer in Brazil include breast, prostate, lung, and colorectal cancers, among others, with incidence rates varying across different regions and populations [9-11].
| Materials and Methods | ▴Top |
Records of cancer deaths in Brazil and the data used
The Mortality Information System (SIM) is an official national epidemiological surveillance system, aimed at capturing data on the country’s deaths to provide mortality information for all health system instances [12]. It is managed by the Health Surveillance Secretariat of the Brazilian Ministry of Health. This system was created in 1975 to collect data on mortality in the country. It has variables that allow, from the cause of death attested by the doctor, to build indicators and process epidemiological analyses that contribute to the efficiency of health management. Deaths from cancer enter the SIM with their cause of death attested and filled in with the description of the malignant neoplasm that caused the respective death.
The population data for the entire Brazilian territory and its five geographic regions come from the database of the Brazilian Institute of Geography and Statistics (IBGE) and are results of demographic censuses conducted.
Both databases (SIM and IBGE) are official databases of the Brazilian State with a history of providing and producing high-quality data. For this reason, they were used as sources for the information contained in this research, without the need for any statistical treatment.
Methodology
The data obtained from DATASUS represents the cumulative number of cancer deaths for each year, up to December 31 of the same year, from 1979 to 2021. Similar data retrieval methods were applied for malignant neoplasms of the breast and prostate.
All information was categorized by gender, with the exception of prostate cancer, and by the five geographic regions of Brazil. Thus, for each base year, the total number of deaths for both men and women in each geographical region was obtained. The sum of these values provided the overall gender-specific data for total cancer deaths in Brazil. After acquisition, this information was presented in the charts in the Data section.
The mortality rates calculated for Brazil were obtained by dividing the total number of cancer deaths each year (total deaths and by gender) by the total number of the Brazilian population, expressed per 100,000 of the population, for the respective year. The mortality rate per 100,000 of USA and China are research data [13-15].
In order to understand the behavior of both mortality and total numbers of deaths from cancer, the concept of growth rate was explored. The growth rate of deaths in a given year was calculated by subtracting the number of deaths in that year (a) from the number of deaths in the previous year (b). The result of this subtraction was then divided by the number of deaths in the previous year (b), expressed as Tc% = (a - b)/b as a percentage relative to the previous year. The sign of this rate indicates an increase (Tc > 0) or decrease (Tc < 0) in number of deaths in relation to the previous year, while its absolute value measures the comportment of these variations.
The values obtained in the growth rate calculations vary from year to year, making it challenging to analyze their trends. To facilitate comparison and understand their respective trends, polynomial interpolation of these values was performed, using second-degree polynomials for analysis, comparison, and presentation of this information.
The graph serves as a visual aid to comprehend the trajectory and trends in cancer-related mortality over the specified period (1979 - 2021). The interpolating polynomial facilitates a smoother interpretation of the growth rates, enhancing the understanding of the overall patterns and fluctuations in cancer deaths over the years in Brazil, as represented in Figure 1 for all neoplasm, as for breast and prostate cancer.
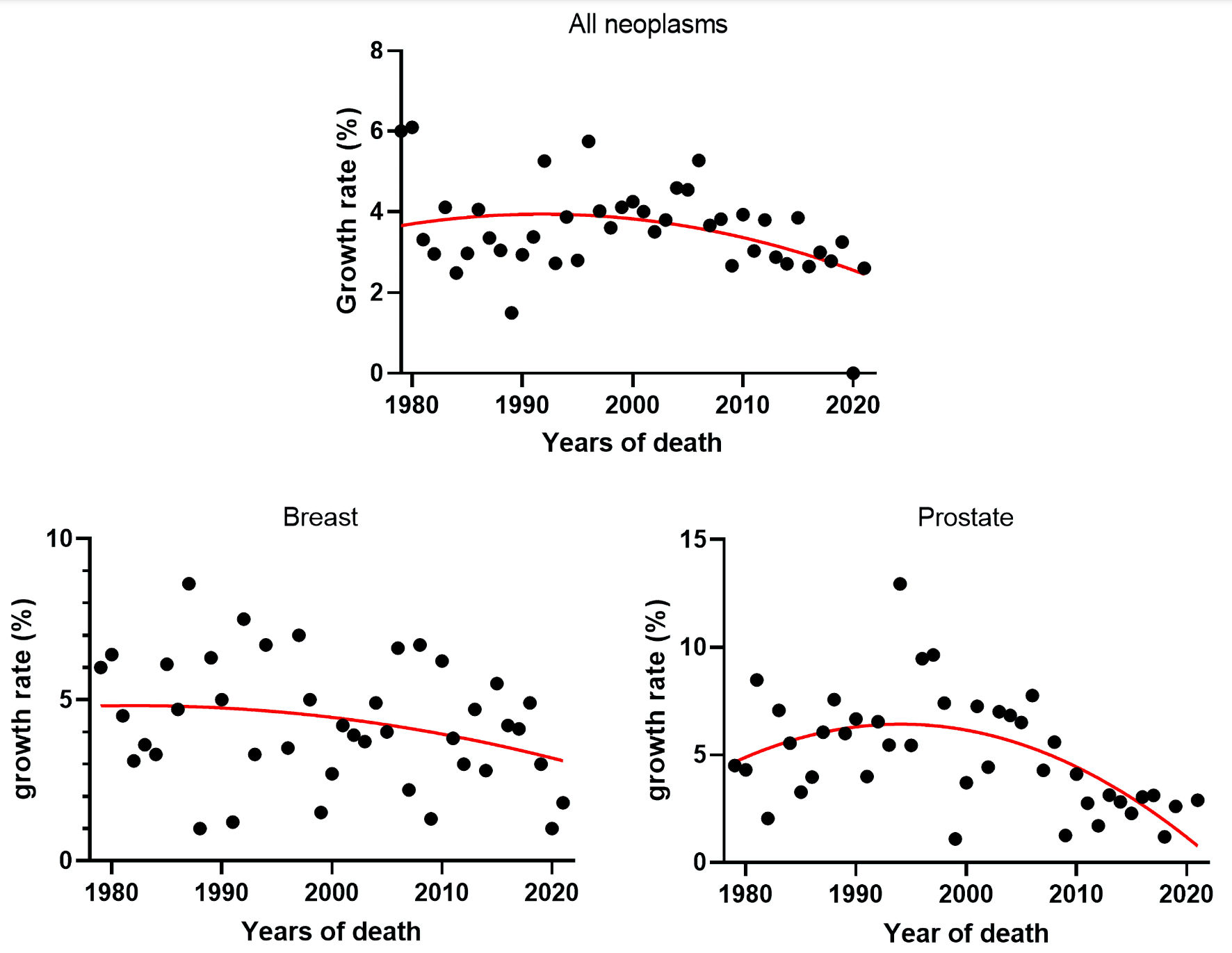 Click for large image | Figure 1. Growth rates of cancer deaths in Brazil from 1979 to 2021 for all neoplasm, breast and prostate cancer and their respective interpolating polynomial. |
Data
Mortality rates are a better indicator of progress against cancer than incidence or survival rates because they are less affected by biases that result from changes in detection practice [16]. The Brazilian cancer mortality data indicate that the male mortality rate is, on average, 20% higher than the female mortality rate. Figure 2 presents the number of deaths from all cancer neoplasms, divided by gender, utilizing data from across Brazil and its five regions for the period from 1979 to 2021.
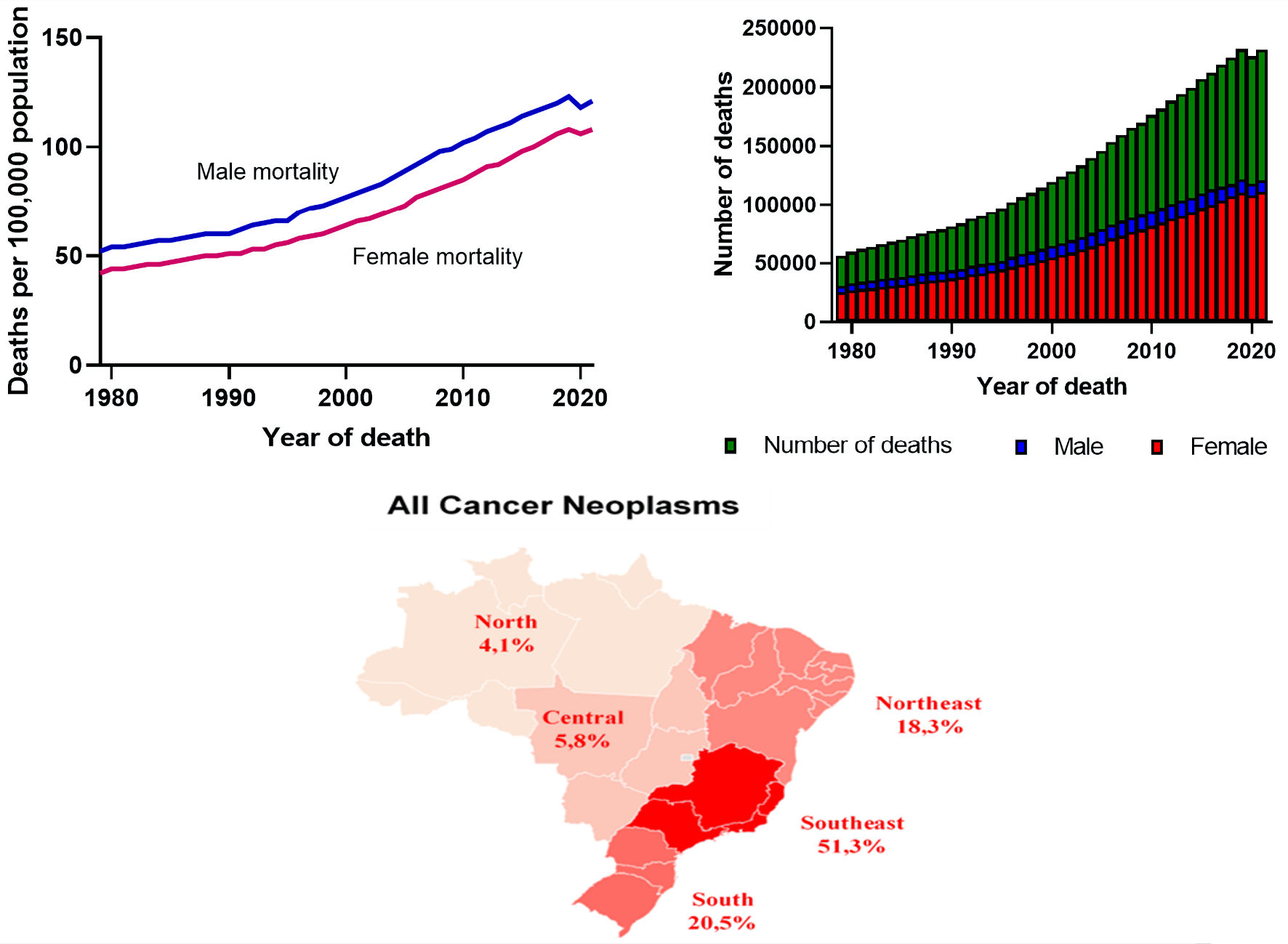 Click for large image | Figure 2. Cancer mortality rates and the distribution of cancer deaths by gender in Brazil, spanning from 1979 to 2021, along with the percentage distribution of these deaths across the five regions. |
The increase in cancer deaths follows the growth of Brazil’s population, albeit at a different growth rate. From 1979 to 2021, while the Brazilian population grew at an average rate of 2.2% per year, the average growth rate of cancer deaths was approximately 12% per year. It is important to note that the calculation for obtaining an average rate was based on a linear progression of both variables. However, the number of deaths from malignant neoplasms does not increase at constant rates, possessing variable actual growth rates. On average, 54% of cancer deaths are in males and 46% in females, resulting in an 8% higher number of deaths in males.
The distribution of cancer deaths (Fig. 3) does not occur uniformly across the five Brazilian geographic regions. The Southern and Southeastern regions lead in the number of deaths, accounting for 20.5% and 51.3% of national deaths from malignant oncological neoplasms, followed by the Northeast with 18.3%, the Central-West with 5.8%, and the North with the lowest national rate at 4.1%.
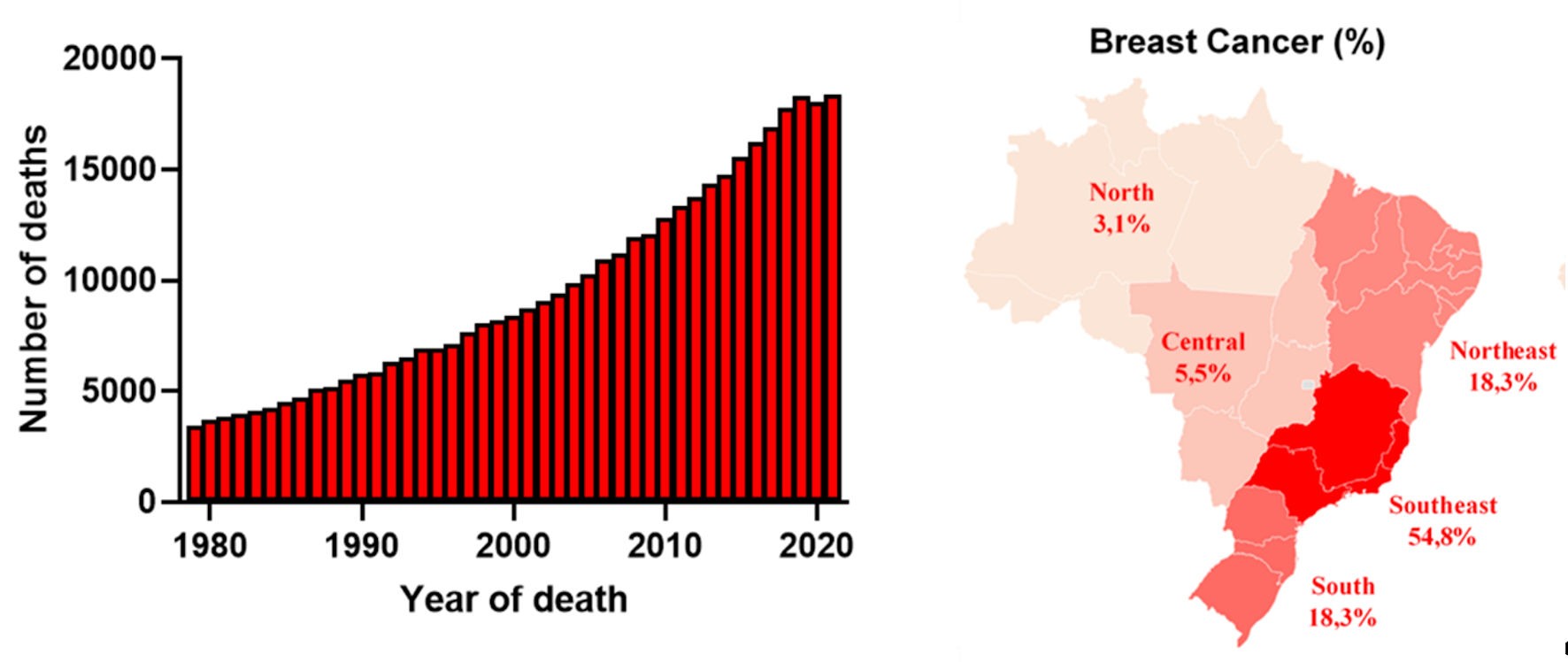 Click for large image | Figure 3. Total deaths from breast cancer in Brazil, along with the percentage distribution of these deaths across the five regions. |
Mirroring the trends observed for all malignant neoplasms, the specific data compiled for breast cancer herein illustrate the total number of deaths attributed to this neoplasm in Brazil from 1979 to 2021, encompassing the aggregate data from its five geographic regions (Fig. 3).
The data indicate that the incidence of breast cancer in women is much higher than in men, representing an average of 99% of deaths recorded from the disease since 1979. However, although representing only an average of 1% of cases, the number of male deaths has been increasing at a rate greater than that of females. While the number of female deaths increases at an average growth rate of 4% per year, the increase in male deaths grows at twice that rate, approximately 8% per year.
The data for deaths from malignant prostate neoplasms, presented here, follow a pattern similar to that of breast cancer data, spanning from 1979 to 2021. Additionally, the distribution of these deaths across the five Brazilian geographic regions is depicted, as detailed in Figure 4.
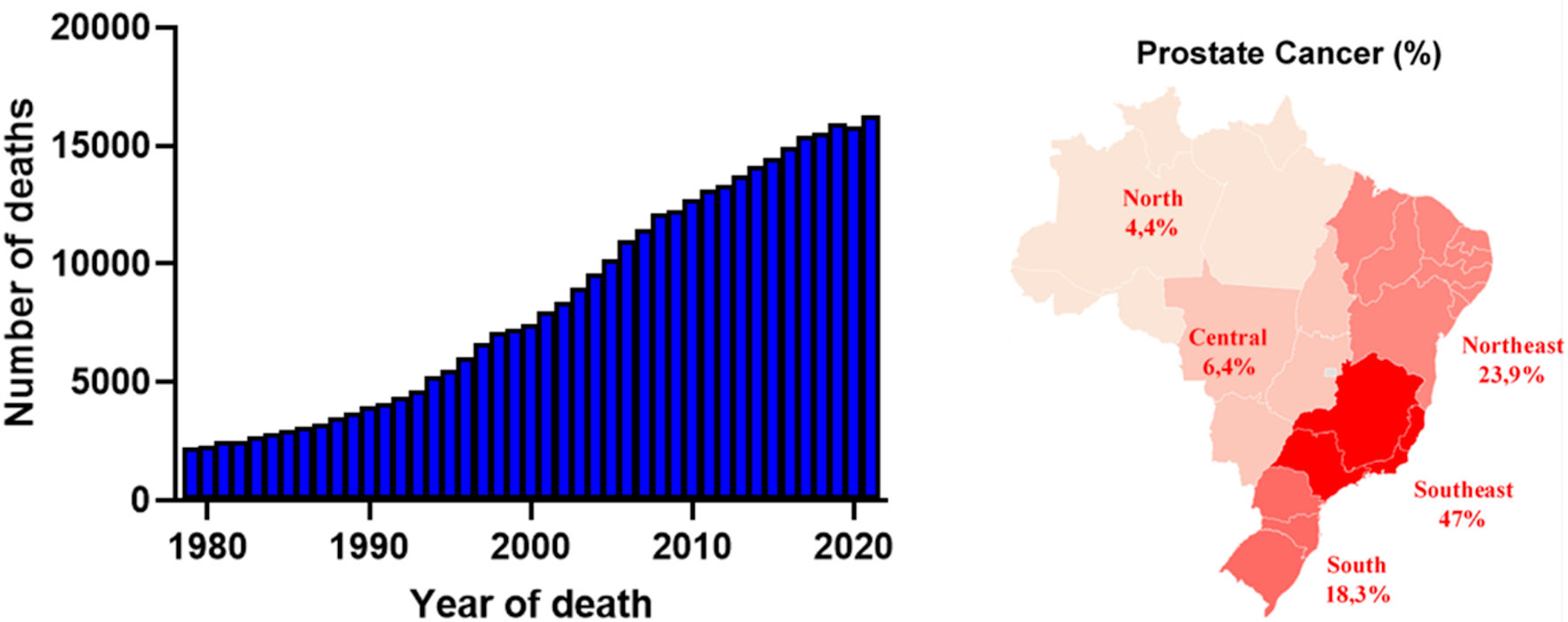 Click for large image | Figure 4. Total deaths from prostate cancer in Brazil, along with the percentage distribution of these deaths across the five regions. |
During this period, approximately 12% of male deaths in Brazil were due to malignant cancer neoplasms, with an average of 6% occurring due to prostate cancer. Since 1979, 362,079 male deaths from this disease have been recorded, with an average growth rate until 2021 of 4.9% per year.
The comparison between the Brazilian, Chinese, and American mortality rates (Fig. 5) shows that the American rate has been experiencing a continuous decline since the 1990s, thus presenting a negative growth rate. It was surpassed in the last decade by the Chinese death rate. Although they are trending upwards, both the Brazilian and Chinese rates have positive growth rates. However, the Brazilian and Chinese mortality rates exhibit differences that extend beyond their absolute values; the Brazilian rate is increasing at a less accelerated pace. This trend of slower growth over the last 15 years will be discussed in more detail later.
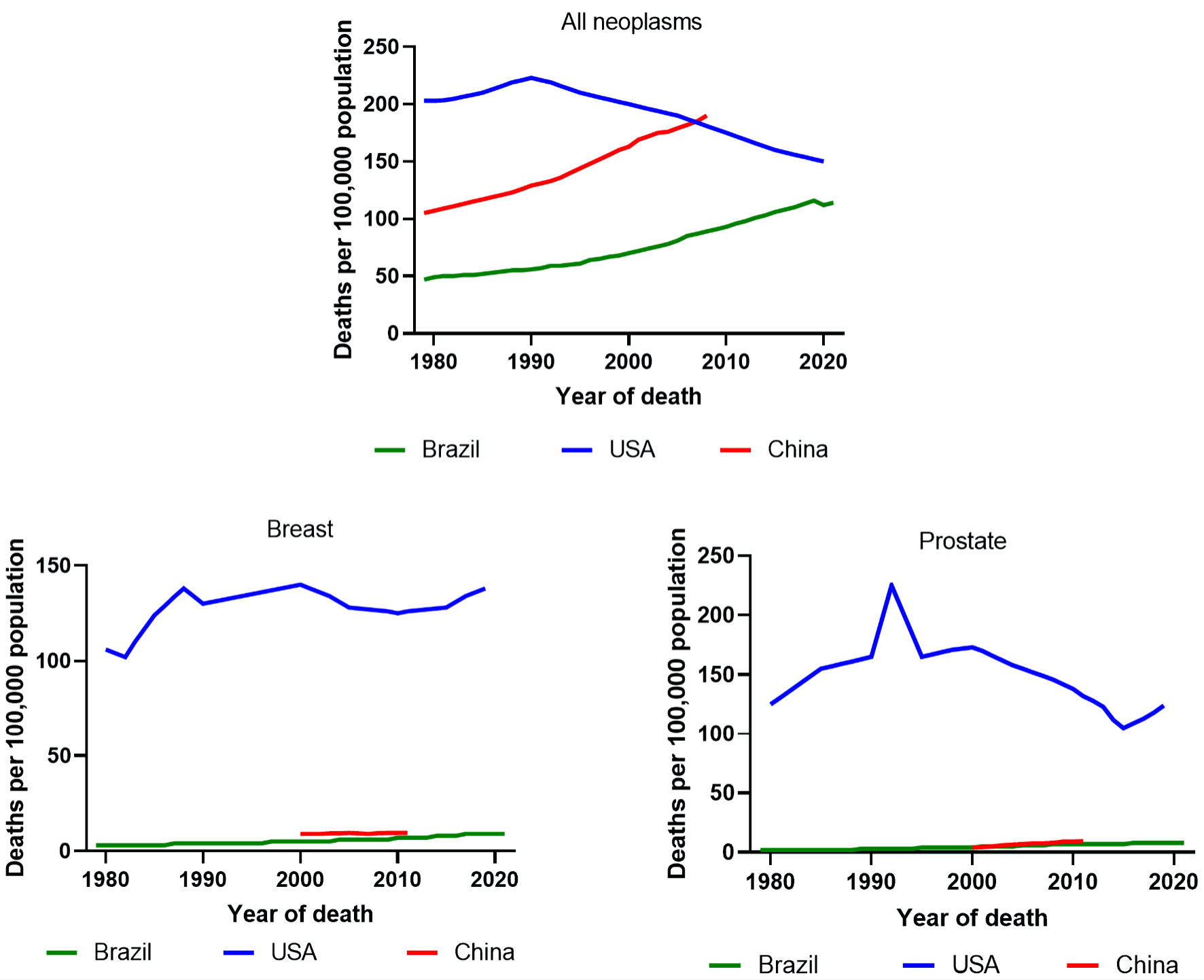 Click for large image | Figure 5. The trends in cancer mortality rates in the USA (1979 - 2019), China (1990 - 2019), and Brazil (1979 - 2021) for all neoplasms, with a specific focus on breast and prostate cancer. |
The comparison of breast cancer mortality rates across Brazil, China, and the USA reveals significant disparities, particularly in the higher American rates. In contrast, the rates in Brazil and China display both a similar trend and similar absolute values. A parallel pattern is observed in prostate cancer mortality rates, with a notable moderation in growth rate during the 2000s, followed by an increase towards the end of the 2020 decade.
The requirement for Institutional Review Board approval and ethical compliance with human study protocols does not apply in this context.
| Results | ▴Top |
The information obtained from 1979 to 2021, after appropriate mathematical treatment, allows us to conduct a series of analyses and comparisons. These not only depict the current reality of cancer death rates in Brazil but also enable a historical analysis of such data. Moreover, it facilitates comparisons across different types of neoplasms and regions, offering insights into the effectiveness of national policies regarding prevention, diagnosis, and treatment.
Analyzing data only quantitatively hides a series of important information about behavior and trends. That is why, in addition to detailed and selective research in the databases of the IBGE and the Brazilian Ministry of Health and the subsequent presentation of the total numbers of deaths from cancer and mortality rates per 100,000 population, with the graphs presented in the section of Data, this article also proposes a data analysis based on the already presented concept of growth rate. The intention of this assessment is to generate understanding about how these numbers increase.
From a simple comparative analysis of the data, it is observed that the total number of cancer deaths increases in almost all the years covered by the study, with the sole exception of 2020, the peak year of the coronavirus disease 2019 (COVID-19) pandemic. It is believed that the high number of deaths among oncology patients due to complications caused by the COVID-19 virus led to the decrease in the registration of cancer deaths. However, to gain more insights into these findings, we will use the concept of annual mortality growth rates due to cancer, as previously presented in the methodology section, to understand how they evolve.
Until now, comparisons were made using average rates, which were based on the linear progression of some quantities and average values of other measures obtained by simply calculating their arithmetic means. However, as mentioned earlier, the actual rates have non-uniform variations with distinct values over the years studied. These seemingly random fluctuations exhibit a trend line, obtained through the interpolations described in the presented methodology.
The analysis of these generated polynomials and the comparison between them enabled a clearer understanding of how the quantity of deaths behaves for both all malignant neoplasms and specific ones. In Figure 6, a comparison is presented between the interpolating polynomials of the growth rates of deaths for all malignant neoplasms and for breast and prostate neoplasms. It is noticeable that although positive, all of them show a decrease in their absolute values in the last 15 years, indicating a tendency to decline. This practically demonstrates that the increase in the number of reported deaths grows in a decelerated manner from this period onward.
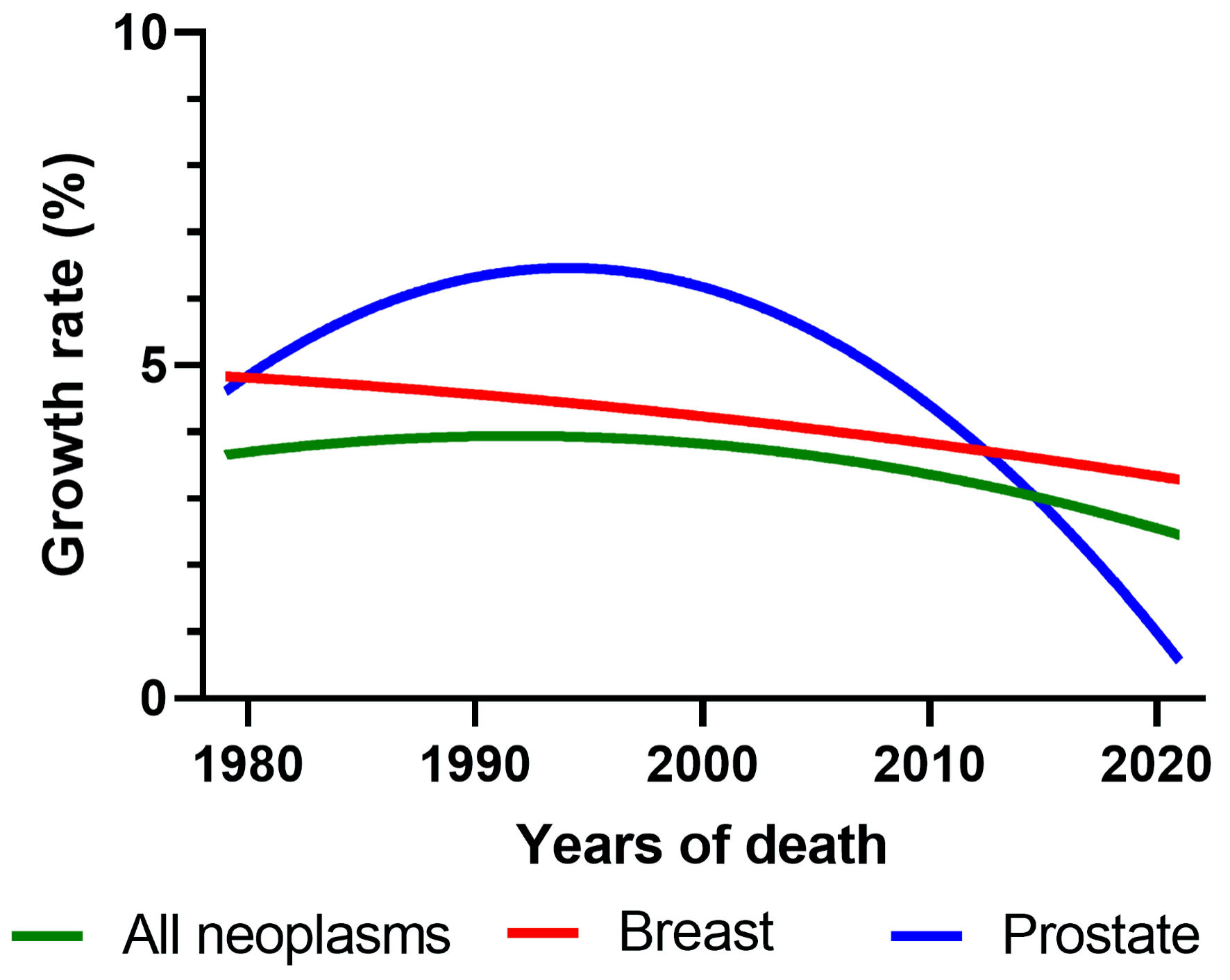 Click for large image | Figure 6. Comparison between the growth rates of cancer deaths in Brazil (all neoplasms, breast, and prostate). |
The comparison between the growth rates of cancer deaths in regional and national rates (Fig. 7) reveals that, although different from each other both in absolute values and behavior, all Brazilian regions follow the national trend, also showing decreasing values over the last 15 years. However, the North and Northeast regions have a delay of ± 5 years in following the same trend.
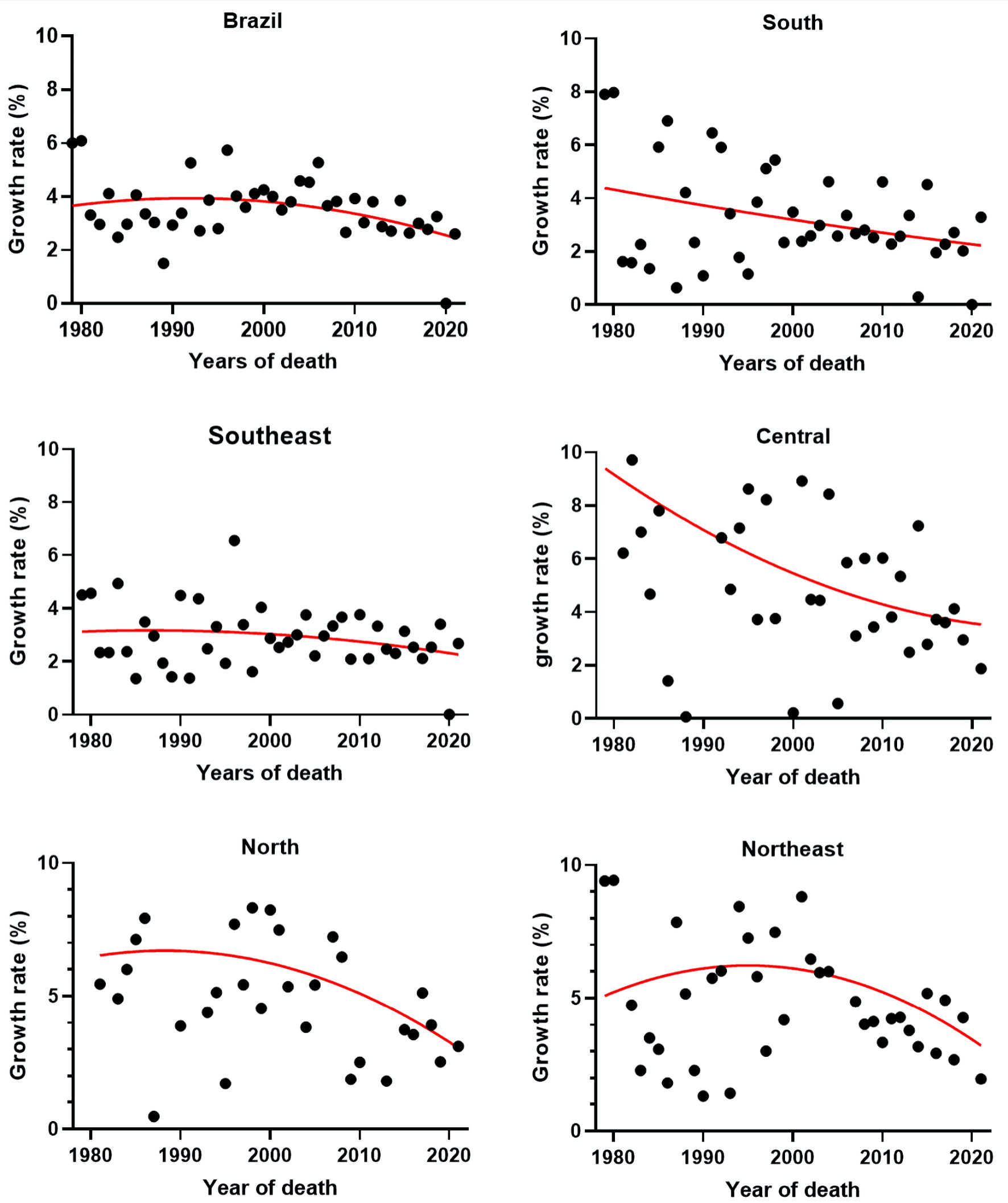 Click for large image | Figure 7. Comparison between the growth rates of cancer deaths in Brazil and its geographic regions. |
The compilation of Brazilian mortality rates for all neoplasms, breast and prostate per 100,000 of the population is shown in Figure 8, and in all of them the trend of slowed growth is notable.
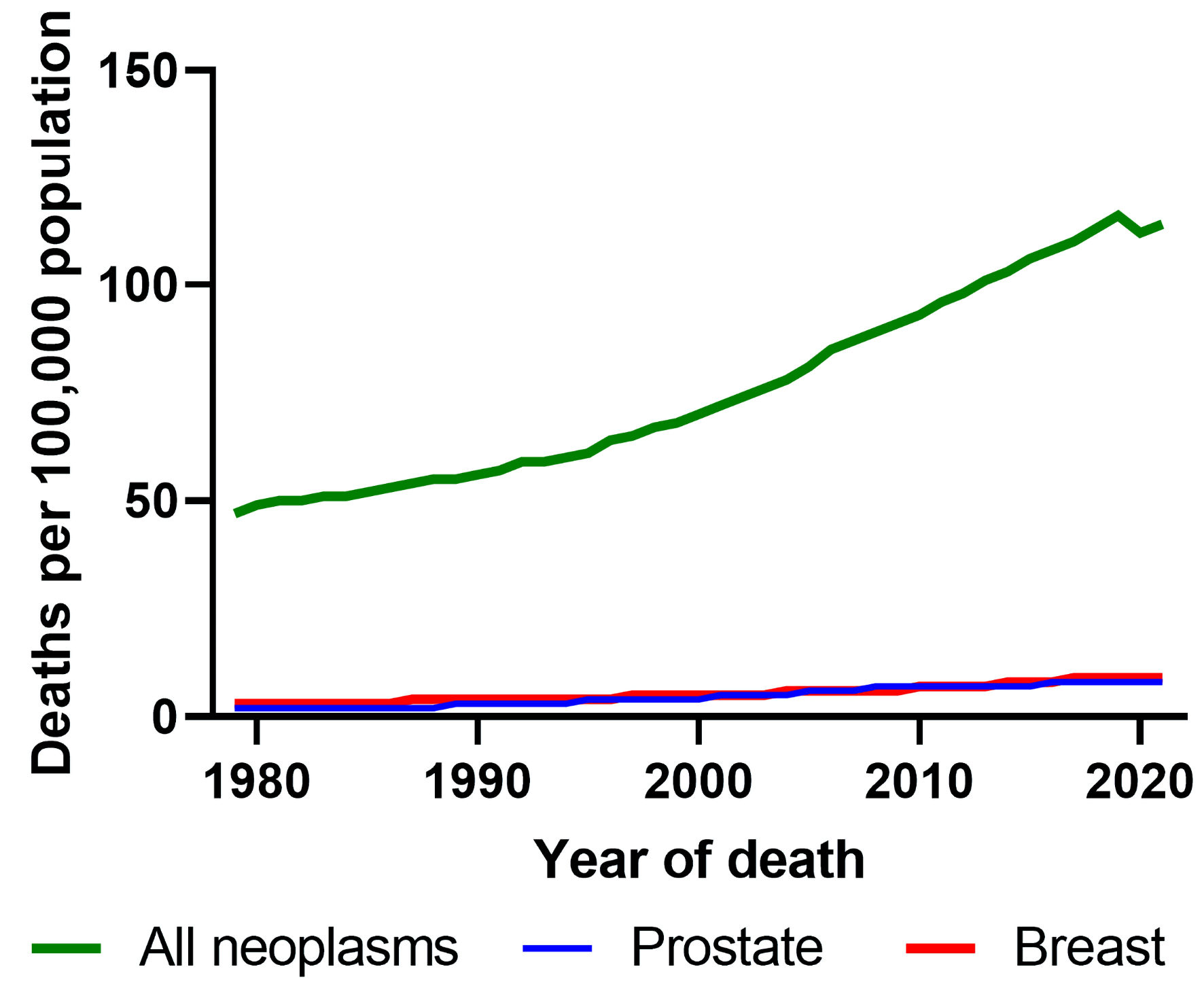 Click for large image | Figure 8. Trends in cancer mortality rates for all cancers, prostate and breast cancer in Brazil (1979 - 2021). |
| Discussion | ▴Top |
In Brazil, the first systematic educational actions regarding cancer prevention emerged in the 1940s. During this time, the need to expand efforts in the fight against cancer led to the creation of the National Cancer Service (SNC), whose objectives were to organize, guide, and control the disease in the country. However, at that moment, educational campaigns aimed to instill notions of protection against the disease through fear and concern. The concepts of “dread” and “announced death” found in most educational materials, were gradually replaced by the idea that resources were available, and there were advancements in the treatment of the disease. The campaigns sought to alert society about the illness without alarming the population. The emphasis on early detection gained strength, propelled by progress in understanding the disease and new treatments. Thus, the health promotion guidelines in the early 1990s brought the understanding of health as a consequence of factors related to the quality of life.
In 2000, the Brazilian National Cancer Institute (INCA) gained the competence to develop “national actions for cancer control”, becoming a national reference for the provision of oncological services under the SUS [17]. Since then, a series of campaigns based on strategies for prevention, screening and early detection, treatment, and palliative care have been implemented. Common modifiable risk factors for cancer, such as smoking, harmful alcohol use, lack of healthy eating habits, and regular physical activity, have also been targets of cancer prevention policies.
Other specific risk factors for cancer, including chronic infections such as those caused by the human papillomavirus (HPV) and hepatitis B and C, in addition to usual preventive campaigns, also involve actionable interventions through extensive free vaccination schemes and effective drug treatments for curing hepatitis C. Governmental approaches with legislation, regulation, and combined fiscal policies have also been part of the national strategy to combat and prevent cancer. Examples of these measures include the taxation of tobacco products and the use of labels with anti-smoking advertisements on them.
In addition to the evolution of preventive measures, significant steps have been taken to increase the national network of oncological care and treatments. In 1998, with the creation of the SUS, the organization of high-complexity oncological hospital care was initiated [17]. In 2000, the creation of the high-complexity assistance centers (CACONs) aimed to decentralize and further increase the care for cancer patients throughout Brazil. However, these institutions, as well as INCA and some university and research institutions dedicated to the care of cancer patients, did not have a specific policy for this activity from the Ministry of Health, nor were there policies focused on professional qualification and differentiated remuneration for these specific activities. In 2005, another important step was taken to increase, organize, and improve the network of treatments with the creation of the National Policy for Oncological Care [18]. This measure aimed to regulate and organize actions for the assistance of cancer patients under SUS, as well as to articulate them with strategies for promotion, prevention, and early detection, and also with the country’s policies for research and scientific and technological development. Such measures significantly expanded access in Brazil to key cancer treatments, including surgery, chemotherapy, and radiotherapy. It is also important to highlight advances in therapeutic techniques and the inclusion of new treatments such as hormone therapy, targeted therapy, and, especially, the advances in immunotherapy over the last decade, involving the use of immunobiologics in cancer combat, which is considered a major therapeutic step [19].
The proposed data analysis through the calculation of cancer death growth rates, along with the observation of their respective trend lines obtained by interpolating the results, proves to be effective mathematical tools for identifying and examining the real impacts that all these measures taken by the Brazilian state, along with current scientific advances, have had on cancer mortality and its neoplasms, especially in breast and prostate cancers. It also allows for a regional perspective. The set of measures taken in the late 1990s, with preventive campaigns and efficient state policies, coupled with research and the development of new therapies, has been responsible for the systematic decline in cancer death growth rates in Brazil over the last 15 years. It has also contributed to the decrease in breast and prostate cancer death growth rates. Although this effect is observed in all national regions, the Northern and Northeastern regions show a delay in following the downward trend, as previously reported.
Conclusions
The data showed that with the drop-in growth rates, the Brazilian mortality rates show a tendency to stabilize, most likely due to massive prevention campaigns and sanitary actions triggered by cancer control policies. This factor becomes more evident in the 2000s, with the maintenance of public cancer prevention policies, as well as an increase in systematic therapy with the introduction of new medications and more sensitive detection exams.
Using breast and prostate cancer as comparative interfaces to assess individualized behavior in subgroups of the disease, the same pattern is observed, supporting a not general, but a systematic trend of reducing the cancer mortality rate in Brazil.
Despite population growth, there is an observed stable, albeit high, mortality rate with a decreasing trend, proving that systematic actions in both cancer prevention and control contribute to maintaining a population’s mortality rate.
Acknowledgments
None to declare.
Financial Disclosure
This study was funded by the Carlos Chagas Filho Foundation for Research Support of Rio de Janeiro State (FAPERJ) (“Scientist of Our State”: E-26/200.815/2021; “NanoHealth Network”: E-26/010.000981/2019, “Research at UEZO”: E-26/010.002362/2019; “Themes”: E-26/211.269/2021, “Infrastructure and Research at UEZO and UERJ”: E-26//211.207/2021, and “Senior Postdoctoral Grant” (PDS): E-26/202.320/2021); and by the National Council for Scientific and Technological Development (CNPq): “Productivity Grant 1B”: 301069/2018-2 to Ralph Santos-Oliveira.
Conflict of Interest
None to declare.
Informed Consent
Not applicable.
Author Contributions
Leonardo Pires Paredes: data curation; formal analysis: investigation, methodology; resources; software; validation; visualization; roles/writing - original draft; writing - review and editing. Marlon da Silva Brandao Rodrigues: data curation; formal analysis; investigation methodology; visualization; roles/writing - original draft. Ralph Santos-Oliveira: conceptualization; data curation; funding acquisition; investigation; methodology; project administration; resources; supervision; visualization; roles/writing - original draft; writing - review and editing.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Dore NI, Teixeira AC. Brazil’s economic growth and real (div)convergence from a very long-term perspective (1822-2019): An historical appraisa. Brazilian Journal of Political Economy. 2022;42(4):934-956.
doi - The World bank. Data Brazil. Acessed December 20, 2023. https://data.worldbank.org/country/BR.
- Roman A. A closer look into Brazil's healthcare system: what can we learn? Cureus. 2023;15(5):e38390.
doi pubmed pmc - Sanders D, Chopra M. Implementing comprehensive and decentralised health systems: the quest for integrated care in post-apartheid South Africa. Int J Integr Care. 2001;1:e33.
pubmed pmc - Araujo JL, Oliveira KKD, Freitas RJM. In defense of the Unified Health System in the context of SARS-CoV-2 pandemic. Rev Bras Enferm. 2020;73(Suppl 2):e20200247.
doi pubmed - Massuda A, Hone T, Leles FAG, de Castro MC, Atun R. The Brazilian health system at crossroads: progress, crisis and resilience. BMJ Glob Health. 2018;3(4):e000829.
doi pubmed pmc - Boccolini CS, de Souza Junior PR. Inequities in Healthcare utilization: results of the Brazilian National Health Survey, 2013. Int J Equity Health. 2016;15(1):150.
doi pubmed pmc - Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7-33.
doi pubmed - Fonseca BP, Albuquerque PC, Saldanha RF, Zicker F. Geographic accessibility to cancer treatment in Brazil: A network analysis. Lancet Reg Health Am. 2022;7:100153.
doi pubmed pmc - da Silva MJS, O'Dwyer G, Osorio-de-Castro CGS. Cancer care in Brazil: structure and geographical distribution. BMC Cancer. 2019;19(1):987.
doi pubmed pmc - Silva GAE, Jardim BC, Ferreira VM, Junger WL, Girianelli VR. Cancer mortality in the Capitals and in the interior of Brazil: a four-decade analysis. Rev Saude Publica. 2020;54:126.
doi pubmed pmc - Brazilian Ministry of Health - National Health Foundation. Mortality information system procedure manual. 2001. Acessed December 21, 2023. https:// https://bvsms.saude.gov.br/bvs/publicacoes/sis_mortalidade.pdf.
- Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, Jemal A, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115-132.
doi pubmed - Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2022. CA: A Cancer Journal for Clinicians. 2023;73(1):17-48.
doi - Xu Q, Zhou M, Yin P, Jin D. Projections of cancer mortality by 2025 in central China: A modeling study of global burden of disease 2019. Heliyon. 2023;9(2):e13432.
doi pubmed pmc - Welch HG, Schwartz LM, Woloshin S. Are increasing 5-year survival rates evidence of success against cancer? JAMA. 2000;283(22):2975-2978.
doi pubmed - Brazilian Ministry of Health. Ordinance n°3535 of September 2, 1998. Accessed December 22, 2023. https://bvsms.saude.gov.br/bvs/saudelegis/gm/1998/prt3535_02_09_1998_revog.html.
- Brazilian Ministry of Health. Ordinance n°874 of May 16, 2013. Accessed December 22, 2023. https://bvsms.saude.gov.br/bvs/saudelegis/gm/2013/prt0874_16_05_2013.html.
- Brazilian Nacional Academy of Medicine. Accessed December 22, 2023. https://www.anm.org.br/imunoterapia-custo-acesso-e-efetividade.
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Oncology is published by Elmer Press Inc.