

| World Journal of Oncology, ISSN 1920-4531 print, 1920-454X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Oncol and Elmer Press Inc |
| Journal website https://www.wjon.org |
Original Article
Volume 15, Number 4, August 2024, pages 675-681

Use of Period Analysis to Timely Assess Five-Year Relative Survival for the Patients With Bone Cancer
Xian Kuan Xiea, i, Xiao Jiao Zhaob, c, i, Run Hua Lic, d, Yong Ran Chenge, Xin Bingb, c, Jun Yangb, Liang You Wangf, Hui Jun Zhug, j, Tian Hui Chenc, d, j, Jin Fei Chenh
aDepartment of Orthopedics, The Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou 310053, China
bSchool of Public Health, Hangzhou Normal University, Hangzhou 311121, China
cDepartment of Cancer Prevention, Zhejiang Cancer Hospital, Hangzhou 310022, China
dHangzhou Institute of Medicine (HIM), Chinese Academy of Sciences, Hangzhou 310018, China
eSchool of Public Health, Hangzhou Medical College, Hangzhou 311399, China
fDepartment of Non-Communicable Chronic Disease Control and Prevention, Taizhou Municipal Center for Disease Control and Prevention, Taizhou 318000, Zhejiang Province, China
gCadre Health Center of Taizhou City, Taizhou 318000, Zhejiang Province, China
hThe First Affiliated Hospital of Wenzhou Medical University, Wenzhou 325000, China
iThese authors contribute equally to this work.
jCorresponding Author: Hui Jun Zhu, Cadre Health Center of Taizhou City, Taizhou 318000, Zhejiang Province, China; Tian Hui Chen, Department of Cancer Prevention, Zhejiang Cancer Hospital, Hangzhou 310022, China
Manuscript submitted March 25, 2024, accepted May 13, 2024, published online July 5, 2024
Short title: Five-Year RS for Bone Cancer Patients
doi: https://doi.org/10.14740/wjon1875
| Abstract | ▴Top |
Background: While timely assessment of long-term survival for patients with bone cancer is essential for evaluation on early detection and prognosis level of treatment of bone cancer, those data are extremely scarce in China. We aimed to timely and accurately assess long-term survival for patients with bone cancer in Eastern China.
Methods: Patients diagnosed with bone cancer during 2004 - 2018 from four cancer registries with high-quality data from Taizhou, Eastern China were included. Five-year relative survival (RS) of bone cancer patients was calculated by period analysis for overall and the stratification. We further predicted 5-year RS during upcoming 2019 - 2023 using a model-based period analysis and survival data during 2004 - 2018.
Results: Overall, 5-year RS for patients with bone cancer during 2014 - 2018 reached 46.6%, being 40.8% for male and 51.0% for female. Five-year RS declined along with aging, decreasing from 58.9% for age < 45 years to 41.5% for age > 60 years, while 5-year RS for urban area was higher compared to rural area (59.1% vs. 44.3%). The 5-year RS during upcoming 2019 - 2023 reached 48.3%. We found a clear upward trend in 5-year RS during 2004 - 2023 for overall and the stratification by sex, age at diagnosis, and region.
Conclusions: We found that, for first time in China using period analysis, most up-to-date 5-year RS for patients with bone cancer reached 46.6% during 2014 - 2018, and is projected to reach 48.3% for the period 2019 - 2023, which has important implications for timely evaluation on early detection and prognosis level of treatment for patients with bone cancer in Eastern China.
Keywords: Bone cancer; Five-year relative survival; Cancer registry; Period analysis
| Introduction | ▴Top |
Bone cancer is a malignant tumor, which originates from limb bones and articular cartilage. While the average age at the onset of bone cancer is young, it accounts for approximately 1% of all cancer-related deaths [1, 2]. It was estimated that overall, 25,800 new cases and 18,400 deaths of bone cancer occurred in 2016 in the whole country, with the crude incidence rate reaching 0.96/100,000 and the crude mortality rate reaching 0.8/100,000 in Zhejiang Province, Eastern China [3].
The long-term survival estimate is essential for cancer burden evaluation by using population-based cancer registry data. The 5-year relative survival (RS) is a key index to assess long-term survival of cancer patients, representing overall level of cancer prevention and control in a region. At present, the calculation methods of 5-year RS include cohort method, complete method, and period analysis. However, cohort and complete methods require 5-year follow-up, leading to at least 5-year delay. Period analysis, which does not require 5 years of follow-up data to calculate survival estimates, is the “gold standard” [4-7] for assessing long-term survival in cancer patients using population-based cancer registry data, which was firstly proposed by Hermann Brenner [5] and later in 2006, Brenner further proposed a model-based period analysis to predict future survival using generalized linear models (GLMs) and previous continuous data. However, the application of the period analysis approach in China has been scarce.
For the first time, our research group systematically utilized period analysis and cancer registry data from Eastern China and found that period analysis was superior to traditional cohort and complete methods in providing more accurate and timely long-term survival estimates and stratification by sex, age at diagnosis, region, and latest estimates of cancer site stratification [8]. For example, for bone cancer in the period 2009 - 2013, the 5-year RS derived from period analysis was closer to the observed actual survival rate than the results derived from the complete and cohort methods. Therefore, the application of period analysis in patients with bone cancer is superior to traditional methods.
Therefore, in this study we aimed to provide most up-to-date (during 2014 - 2018) estimates of 5-year RS for bone cancer patients in the Chinese population, using period analysis and population-based cancer registry data from Taizhou, Eastern China. We also aimed to project 5-year RS for the upcoming 2019 - 2023 and to assess trends in 5-year RS from 2004 to 2023, using continuous data during 2004 - 2018 and a model-based period analysis.
| Materials and Methods | ▴Top |
Data source
The data of this study were derived from the Cancer Registry of Taizhou, Eastern China, and the database covered nine cancer registries. According to the standard of “death certificate (DCO) cases accounting for less than 13%” [8], cases from four cancer registries (Luqiao, Yuhuan, Xianju, and Wenling) were included for further analysis, covering a total population of 2.6 million.
The cancer coding was based on the International Classification of Diseases, 10th Revision (ICD-10) and the International Classification of Diseases for Oncology, Third Edition (ICD-O-3). Patients diagnosed with primary bone cancer between January 1, 2004, and December 31, 2018 (using ICD-10 code C40-C41) were included. All bone cancer patients used a combination of active and passive follow-up to determine survival information until the end of 2018. Passive follow-up means that staff of local registries linked the cancer records and death records based on identifiable information. Active follow-up means that patients who cannot be linked to the death surveillance system were followed by regular visit, telephone, letter, and e-mails approaches. IARCcrgTools [8] were used to evaluate data quality after deletion of patients with lost follow-up, secondary cancers, unknown records, missing follow-up time, and then inconsistent data were screened and eliminated. Finally, 434 qualified cases were included as research patients for further analyses.
Institutional Review Board approval
The data use for this study was approved and the written informed consent was exempt by the Institutional Review Board of Zhejiang Cancer Hospital, China (IRB-2023-324). The ethical compliance with human study was not applicable.
Statistical analysis
To compare the distribution differences of basic characteristics of patients in the three periods of 2004 - 2008, 2009 - 2013 and 2014 - 2018, the categorical variables χ2 test was used to analyze the data. P < 0.05 was considered to be statistically significant.
The 5-year RS, the ratio of actual to expected survival rate, was calculated for patients with bone cancer from 2014 to 2018 using period analysis. The expected survival rate was calculated by Ederer II method [4] according to the life table of Taizhou four regions (Luqiao, Wenling, Xianju, and Yuhuan) stratified by sex, age at diagnosis, region and year.
The cases included in the period analysis were divided into two parts, one was newly diagnosed cases during the period of interest (2014 - 2018), and the other was cases diagnosed before the period of interest (2009 - 2013) and still alive during the period of interest. This method was used to process left-censored data diagnosed before the period of interest and right-censored data of patients who were alive after the period of interest [4]. The method involves arranging the data into the form of a life table and calculating the 1-year RS Si at the i year of follow-up. The formula was as follows:
In this formula, ni represented the population at the beginning of the i year of follow-up, di represented the number of deaths at the end of i year of follow-up, and ci represented the number of censored data in i year. The observed survival
RS is the ratio of actual survival rate to expected survival rate. The formula was as follows:
When calculating the 5-year RS, k = 5 was used in the above equation. Where,
Next, model-based period analysis was used to predict the 5-year RS of bone cancer patients in four districts of Taizhou, Eastern China from 2019 to 2023, and patients were stratified according to age at diagnosis, sex, and region. First, according to the principle of the period analysis, the data of the three periods of 2004 - 2008, 2009 - 2013 and 2014 - 2018 are included. Then, the annual follow-up year and follow-up period were used as independent variables, and the conditional 1-year survival rate of each year was used as the dependent variable. Finally, a GLM [9] was built by binomial regression to predict the 5-year RS for the period 2019 - 2023.
| Results | ▴Top |
Basic characteristics of bone cancer patients
The diagnosis of bone cancer patients in Taizhou from 2004 to 2018 is shown in Table 1. The total number of cases was 434, and the number of diagnosed cases of bone cancer increased rapidly from 38 cases in 2004 - 2008 to 253 cases in 2014 - 2018. The number of cases was 252 in males and 182 in females, with a male-to-female ratio of 1.38, which was statistically significant (P < 0.001). The number of cases in urban and rural areas was 119 and 315 respectively, with more cases in rural areas than in urban areas (P < 0.001). The mean age of diagnosis of bone cancer was 61 years old. The number of patients diagnosed at < 45 years old, 45 - 60 years old and > 60 years old were 101, 128 and 205 respectively and the proportion of patients > 60 years old was more than 40%. This distribution was statistically significant from 2004 to 2018 (P < 0.001).
 Click to view | Table 1. Basic Characteristics of Bone Cancer Patients Diagnosed During 2004 - 2018 in Taizhou, Eastern China |
Five-year RS of the bone cancer patients
As shown in Table 2, the 5-year RS of patients with bone cancer, during 2014 - 2018 was 46.6%. The 5-year RS was stratified by age, sex and region. The results showed that the 5-year RS of male and female patients were 40.8% and 51.0%, respectively. The 5-year RS of urban patients with bone cancer was higher than that of rural patients (59.1% vs. 44.3%). The 5-year RS of patients aged < 45, 45 - 60 and > 60 years was 58.9%, 45.8% and 41.5%, respectively.
Click to view | Table 2. Five-Year Relative Survival During 2014 - 2018 for Patients With Bone Cancer From Taizhou, Eastern China |
Projected 5-year RS during the upcoming 2019 - 2023 and the trend during 2004 - 2023
As shown in Table 3, by using survival data and model-based period analysis (using a GLM) for three consecutive 5 years (2004 - 2008, 2009 - 2013, and 2014 - 2018), it is predicted that the overall 5-year RS for the next 5 years (2019 - 2023) may reach 48.3% (46.9% for males, 50.8% for females). We also found a clear age gradient for 5-year RS, falling from 63.4% at diagnosis < 45 years to 42.0% at > 60 years. The 5-year RS was higher in urban areas compared to rural areas (62.9% vs. 46.9%). We found a clear upward trend in 5-year RS overall and stratified by sex, age at diagnosis, and region over the period 2004 - 2023 (Figs. 1-3).
Click to view | Table 3. Prediction of 5-Year Relative Survival During Upcoming 2019 - 2023 for Patients With Bone Cancer From Taizhou, Eastern China |
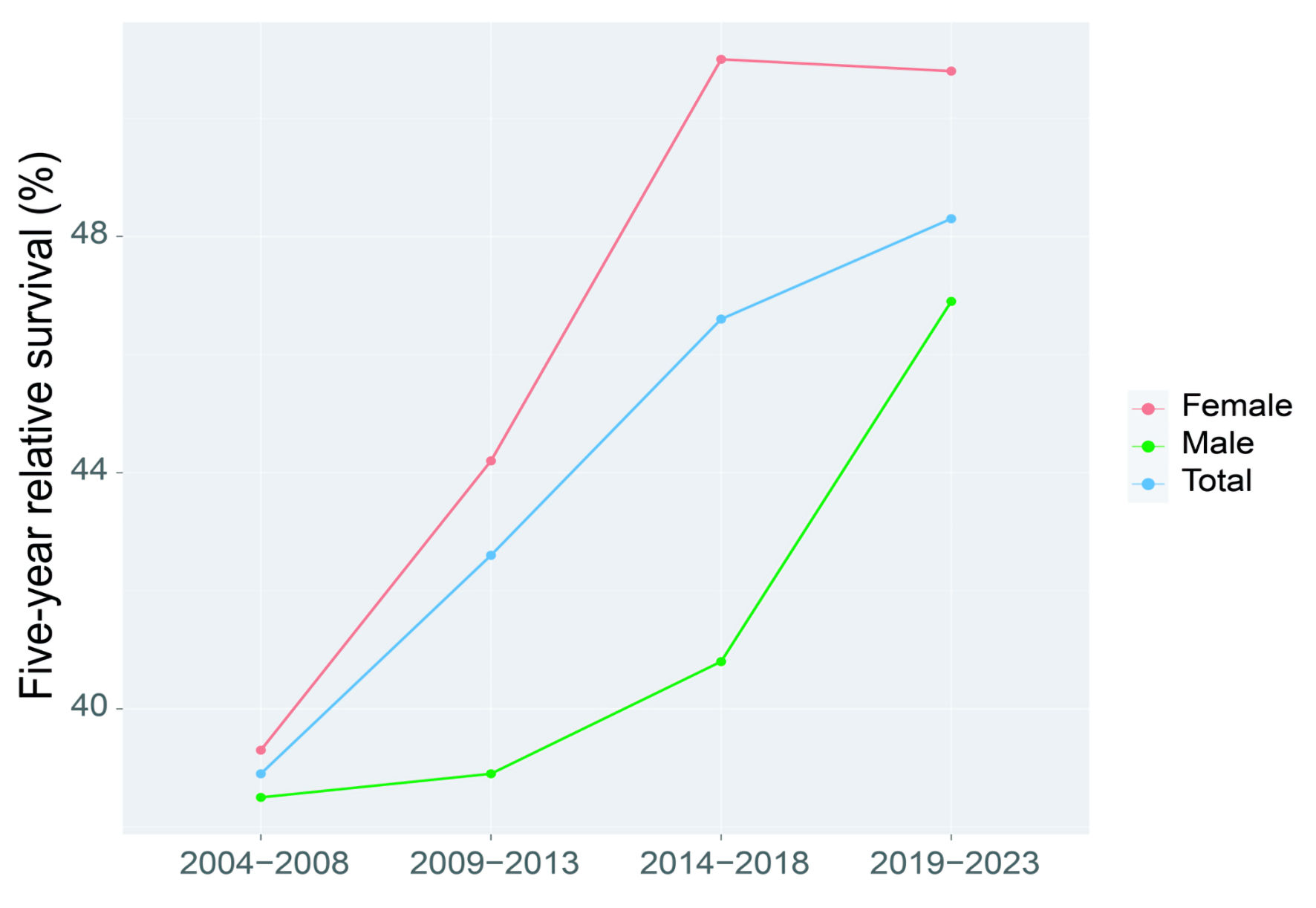 Click for large image | Figure 1. Five-year relative survival for overall and the stratification by sex for patients with bone cancer from Taizhou, Eastern China during 2004 - 2008, 2009 - 2013, 2014 - 2018 and 2019 - 2023. |
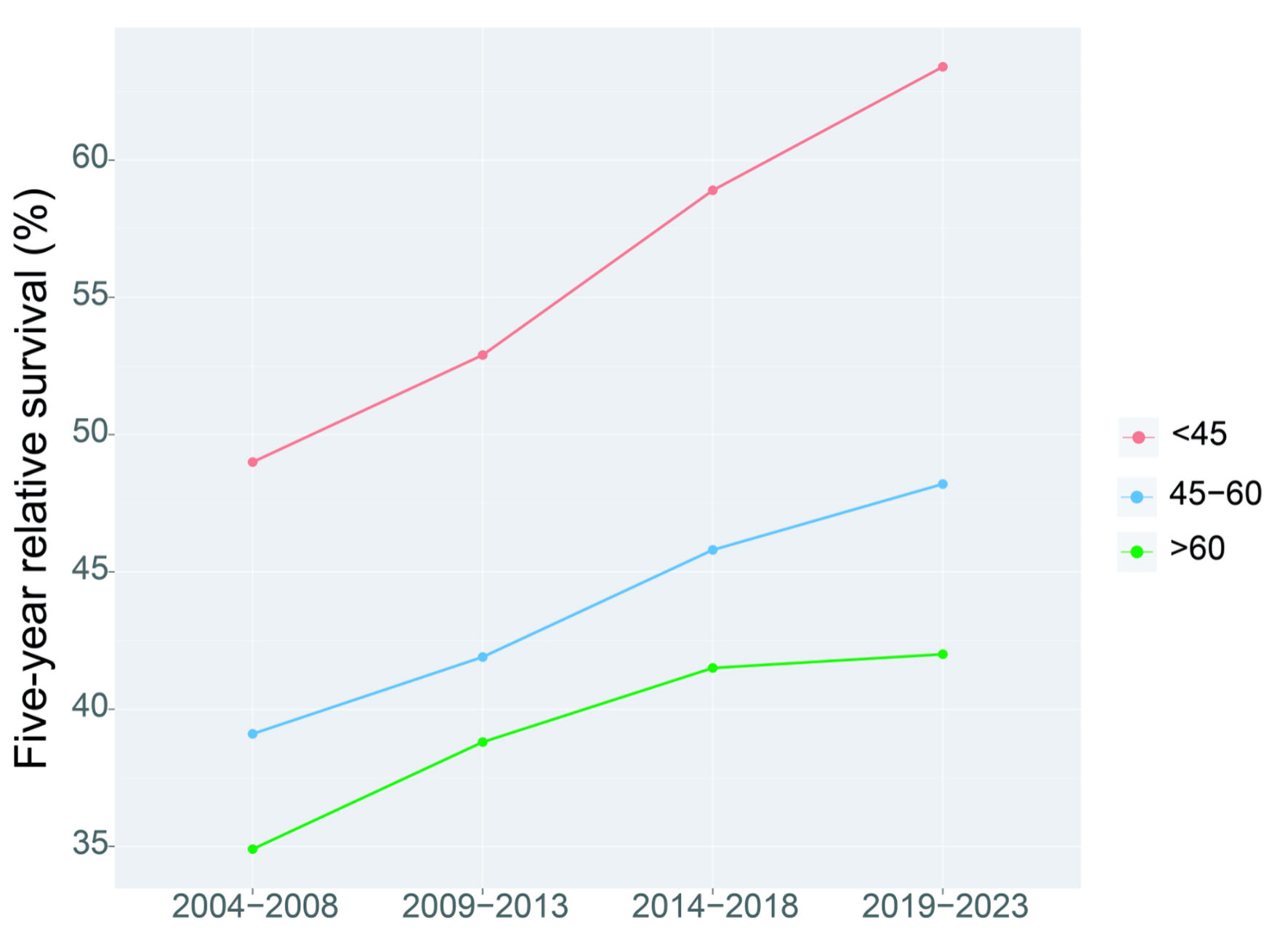 Click for large image | Figure 2. Five-year relative survival for overall and the stratification by age at diagnosis for patients with bone cancer from Taizhou, Eastern China during 2004 - 2008, 2009 - 2013, 2014 - 2018 and 2019 - 2023. |
 Click for large image | Figure 3. Five-year relative survival for overall and the stratification by region (urban and rural areas) for patients with bone cancer from Taizhou, Eastern China during 2004 - 2008, 2009 - 2013, 2014 - 2018 and 2019 - 2023. |
| Discussion | ▴Top |
In our study, 5-year RS of bone cancer in Taizhou reached 46.6% during 2014 - 2018, which was higher than the 26.5% reported in China during 2012 - 2015 [10]. Two reasons could explain the significance of the result. First of all, compared to our data (2014 - 2018), 26.5% of China’s reported calculation period from 2012 to 2015 was 3 years earlier. In recent years, with the progress of science and technology and the improvement of treatment level, it is common knowledge that the survival rate of patients with bone cancer will be improved (our data were 3 years later) [11-13]. Second, 26.5% of the reports in 2012 - 2015 were calculated by the cohort method, which will underestimate the true survival estimate compared to period analysis, as confirmed by our group for the 5-year RS during 2009 - 2013 [8]. Additionally, the report of 26.5% during 2012 - 2015 for China was actually projected rather than estimated. Because the data for the study were from 17 cancer registries only with cancer patients diagnosed until the end of 2013 and followed up until the end of 2015 [10], the 5-year RS for patients with any cancer type including bone cancer could be calculated at the latest for 2013. Nevertheless, other studies have reported that the 5-year survival estimate of patients with bone cancer in Europe, the United States and Japan was higher than that of this study (46.6%), reaching 53%, 59% and 68.4%, respectively [14-16]. Several factors may account for these divergent results. First, in our study, the average age of diagnosis (61.4 years) was too high and the higher the age, the lower the survival rate. This age potentially incorporated cumulative exposure to various risk factors. Second, compared with developed countries, China’s diagnosis and treatment technology is comparatively inadequate, and the level of medical service is relatively moderate. Generally speaking, the 5-year RS in this study is higher than that in China but lower than that in developed countries, which is reasonable.
In this study, 5-year RS of bone cancer patients was further stratified by age at diagnosis, sex, and region. We found that 5-year RS of females was reasonably higher than that of males (51.0% vs. 40.8%), which was consistent with previous studies [13]. This may be related to more smoking and alcohol abuse in males. The incidence of bone cancer in males are higher than those in females, but the survival rate is lower, which may be related to the protective effect of estrogen [17]. It is worth noting that in this study, the increasing trend of female incidence was significantly higher than that of male during 2014 - 2018, similar to that of African Americans, Norway and the Netherlands [17]. We also identified that the 5-year RS in urban areas was higher than that in rural areas (59.1% vs. 44.3%). The reasons are as follows. First, bone cancer is a rare disease, accounting for only 0.2% of all malignant tumors. The biggest problem in the diagnosis and treatment of rare diseases is the poor standardization [18]. Due to the uneven development of regional medical care in China, the problem of non-standardized diagnosis and treatment is particularly prominent. In addition, the limited medical equipment and professional and technical personnel in rural areas further aggravate the unreasonable allocation of urban and rural health resources. Therefore, the overall planning of urban and rural health resources can help to modify the current situation of unreasonable allocation of health resources in China and further improve the level of rural health services [19]. We observed a significant age gradient in 5-year RS among patients with bone cancer, with 5-year RS decreasing from 58.9% < 45 years old to 41.5% > 60 years old. It indicates that young patients have a higher survival rate, which is consistent with other reports [17], and according to common sense, the overall bone function of young people is better than that of the elderly.
Our study found that the overall 5-year increase in RS between 2004 and 2023, and stratification by sex, age at diagnosis, and region is reasonable for the following reasons. First of all, although the progress of clinical treatment is conducive to improving the survival rate of patients with bone cancer, immunochemotherapy is the most effective treatment to improve the survival of patients with bone cancer [20-22]. Second, in recent years, screening methods based on computed tomography (CT), X-ray, magnetic resonance imaging (MRI) and other screening methods have been widely used in routine physical examinations, which can detect abnormalities in most patients with bone cancer [23]. Therefore, the significant improvement in survival of bone cancer in the past 10 years could be attributed to improvements in monitoring, screening, and early detection. Third, Taizhou is a coastal city in Eastern China with rapid economic development and mature medical level and system. Additionally, the improvement in 5-year RS for patients with bone cancer may be partially attributed to the enhancement of health awareness of Taizhou residents, where the awareness rate of core knowledge of cancer prevention and treatment among residents in Zhejiang reaches 78.4% [24].
Our study has some advantages and limitations. Three advantages are listed below. First, we used period analysis for the first time in China to provide the latest (2014 - 2018) 5-year RS for patients with bone cancer in Taizhou, Eastern China. Second, we assessed survival trends and found that 5-year RS for bone cancer patients improved significantly between 2004 - 2008, 2009 - 2013, and 2014 - 2018. Third, we have predicted RS for the next 5 years from 2019 - 2023. However, there are still some limitations. First, we were unable to provide stratified survival data for patients with bone cancer by stage, histology and treatment. Nevertheless, population-based cancer registries commonly do not include clinical information on cancer patient staging (e.g., tumor, node, and metastasis (TNM)), histology, and treatment. Second, we only provide the latest survival data for bone cancer patients in Taizhou, Eastern China. Therefore, further investigations using provincial or national cancer registry data are also highly warranted.
Conclusions
We found that, for first time in China using period analysis, most up-to-date 5-year RS for patients with bone cancer reached 46.6% during 2014 - 2018. The study also revealed that 5-year RS for bone cancer patients have improved greatly during 2004 - 2018, regardless of gender, age at diagnosis, and region at diagnosis, which is essential for the evaluation of early detection and prognosis level of treatment for bone cancer in Eastern China.
Acknowledgments
The authors are grateful to all the staffs of Taizhou Center for Disease Control and Prevention and the four county-level centers (Luqiao, Yuhuan, Xianju, and Wenling) for their kind collaboration and contributions in providing cancer data, data curation, classification, validation, and database creation.
Financial Disclosure
This work was supported by grants from the Ten-Thousand Talents Plan of Zhejiang Province (2021R52020), Zhejiang Province Natural Science Funds Grant (LTGD23H090006) and Joint Key Program of Zhejiang Province-Ministry of Health (WKJ-ZJ-1714). The funding agencies had no role in the design and conduct of the study, collection, management, analysis, and interpretation of the data, preparation, review, or approval of the manuscript, and decision to submit the manuscript for publication.
Conflict of Interest
None to declare.
Informed Consent
Although the data from nine cancer registries from Taizhou, Eastern China were completely anonymous, and their use did not entail ethical problems, the data use for this study were approved and the written informed consent was also exempt by the Institutional Review Board of Zhejiang Cancer Hospital, China (IRB-2023-324).
Author Contributions
Tian Hui Chen was responsible for the study concept and design. Liang You Wang acquired data. Yong Ran Cheng analyzed data. Xiao Jiao Zhao and Xin Bing drafted the manuscript, and all authors revised it for important intellectual content. All authors approved the submission and publication of the manuscript.
Data Availability
The raw data will be available for reasonable request to the corresponding author (TC).
| References | ▴Top |
- Lin HN, Gu XY, Zhang SW, Zeng HM, Wei WW, Zheng RS. [Analysis on incidence and mean age at diagnosis for Global Cancer]. Zhonghua Zhong Liu Za Zhi. 2018;40(7):543-549.
doi pubmed - Zheng R, Zhang S, Zeng H, Wang X, Sun K, Chen R, Li L, Wei W, He J. Cancer incidence and mortality in China, 2016. Journal of the National Cancer Center. 2022;2(1):1-9.
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209-249.
doi pubmed - Brenner H, Gefeller O, Hakulinen T. Period analysis for 'up-to-date' cancer survival data: theory, empirical evaluation, computational realisation and applications. Eur J Cancer. 2004;40(3):326-335.
doi pubmed - Brenner H, Hakulinen T. Up-to-date and precise estimates of cancer patient survival: model-based period analysis. Am J Epidemiol. 2006;164(7):689-696.
doi pubmed - Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Niksic M, Bonaventure A, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. 2018;391(10125):1023-1075.
doi pubmed pmc - Brenner H, Hakulinen T. Period versus cohort modeling of up-to-date cancer survival. Int J Cancer. 2008;122(4):898-904.
doi pubmed - Jiang X, Wang L, Cheng Y, Tang H, Chen T. Assessment of long-term survival of cancer patients using cancer registry data from eastern China: Period analysis is superior to traditional methods. Int J Cancer. 2020;147(4):996-1005.
doi pubmed - Holleczek B, Gondos A, Brenner H. periodR - an R package to calculate long-term cancer survival estimates using period analysis. Methods Inf Med. 2009;48(2):123-128.
doi pubmed - Zeng H, Chen W, Zheng R, Zhang S, Ji JS, Zou X, Xia C, et al. Changing cancer survival in China during 2003-15: a pooled analysis of 17 population-based cancer registries. Lancet Glob Health. 2018;6(5):e555-e567.
doi pubmed - Prasad SR, Kumar TSS, Jayakrishnan A. Nanocarrier-based drug delivery systems for bone cancer therapy: a review. Biomed Mater. 2021;16(4):044107.
doi pubmed - Li Y, Hou H, Zhang P, Zhang Z. Co-delivery of doxorubicin and paclitaxel by reduction/pH dual responsive nanocarriers for osteosarcoma therapy. Drug Deliv. 2020;27(1):1044-1053.
doi pubmed pmc - Sturge J. Endo180 at the cutting edge of bone cancer treatment and beyond. J Pathol. 2016;238(4):485-488.
doi pubmed pmc - Stiller CA, Botta L, Brewster DH, Ho VKY, Frezza AM, Whelan J, Casali PG, et al. Survival of adults with cancers of bone or soft tissue in Europe-Report from the EUROCARE-5 study. Cancer Epidemiol. 2018;56:146-153.
doi pubmed - Smeland S, Bielack SS, Whelan J, Bernstein M, Hogendoorn P, Krailo MD, Gorlick R, et al. Survival and prognosis with osteosarcoma: outcomes in more than 2000 patients in the EURAMOS-1 (European and American Osteosarcoma Study) cohort. Eur J Cancer. 2019;109:36-50.
doi pubmed pmc - Fukushima T, Ogura K, Akiyama T, Takeshita K, Kawai A. Descriptive epidemiology and outcomes of bone sarcomas in adolescent and young adult patients in Japan. BMC Musculoskelet Disord. 2018;19(1):297.
doi pubmed pmc - Ottaviani G, Jaffe N. The epidemiology of osteosarcoma. Cancer Treat Res. 2009;152:3-13.
doi pubmed - Niu XH. [Interpretation of 2020 NCCN clinical practice guidelines in oncology-bone cancer]. Zhonghua Wai Ke Za Zhi. 2020;58(6):430-434.
doi pubmed - Li J, Shi L, Liang H, Ding G, Xu L. Urban-rural disparities in health care utilization among Chinese adults from 1993 to 2011. BMC Health Serv Res. 2018;18(1):102.
doi pubmed pmc - Keil L. Bone Tumors: Primary Bone Cancers. FP Essent. 2020;493:22-26.
pubmed - Jafari F, Javdansirat S, Sanaie S, Naseri A, Shamekh A, Rostamzadeh D, Dolati S. Osteosarcoma: A comprehensive review of management and treatment strategies. Ann Diagn Pathol. 2020;49:151654.
doi pubmed - Miwa S, Shirai T, Yamamoto N, Hayashi K, Takeuchi A, Igarashi K, Tsuchiya H. Current and emerging targets in immunotherapy for osteosarcoma. J Oncol. 2019;2019:7035045.
doi pubmed pmc - Bandyopadhyay O, Biswas A, Bhattacharya BB. Bone-cancer assessment and destruction pattern analysis in long-bone X-ray image. J Digit Imaging. 2019;32(2):300-313.
doi pubmed pmc - You-Qing W, Ling-Bin DU, Hui-Zhang LI, Chen Z, Hui-Juan Z, Center ZCJCC: Survey on awareness of cancer prevention in residents of Zhejiang Province. 2018.
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Oncology is published by Elmer Press Inc.